Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Anatomy of Stretching: Structural LimitationsDocumento5 pagineAnatomy of Stretching: Structural LimitationssdjuknicNessuna valutazione finora
- Energetics and Biomechanics of Inclined Treadmill Walking in Obese AdultsDocumento9 pagineEnergetics and Biomechanics of Inclined Treadmill Walking in Obese AdultssdjuknicNessuna valutazione finora
- Exercise Neuroendokrine Stress PDFDocumento10 pagineExercise Neuroendokrine Stress PDFsdjuknicNessuna valutazione finora
- Consenso Condicionamento Físico (Kraemer)Documento5 pagineConsenso Condicionamento Físico (Kraemer)pedromattarnogueira7734100% (2)
- MARAJA II Do 18.4. Doručak: Ručak Večera Ponedeljak/ČetvrtakDocumento2 pagineMARAJA II Do 18.4. Doručak: Ručak Večera Ponedeljak/ČetvrtaksdjuknicNessuna valutazione finora
- Dosadasnja Naucna AktivnostDocumento13 pagineDosadasnja Naucna AktivnostsdjuknicNessuna valutazione finora
- Fulltext PDFDocumento12 pagineFulltext PDFsdjuknicNessuna valutazione finora
- Viru PlanningOfMicrocyclesDocumento6 pagineViru PlanningOfMicrocyclessdjuknicNessuna valutazione finora
- Trainers Postural Stability & Exercise Technique Part 2Documento4 pagineTrainers Postural Stability & Exercise Technique Part 2sdjuknicNessuna valutazione finora
- Traaniners Postural Stability & Exercise Technique Part 1Documento4 pagineTraaniners Postural Stability & Exercise Technique Part 1sdjuknicNessuna valutazione finora
- Training ExampDocumento1 paginaTraining ExampsdjuknicNessuna valutazione finora
- Floyd17 TB ch13 PDFDocumento5 pagineFloyd17 TB ch13 PDFsdjuknicNessuna valutazione finora
- Walk PDFDocumento8 pagineWalk PDFsdjuknicNessuna valutazione finora
- Verhoshanskyprinciples 1 PDFDocumento8 pagineVerhoshanskyprinciples 1 PDFBrandy MaloneNessuna valutazione finora
- Floyd17 TB Ch07Documento5 pagineFloyd17 TB Ch07sdjuknicNessuna valutazione finora
- The Application of Complex Training For The Development of Explosive PowerDocumento16 pagineThe Application of Complex Training For The Development of Explosive PowersdjuknicNessuna valutazione finora
- 826-3 Bompa Rev 6 2005 InglesDocumento7 pagine826-3 Bompa Rev 6 2005 InglessdjuknicNessuna valutazione finora
- Floyd17 TB Ch12Documento5 pagineFloyd17 TB Ch12sdjuknicNessuna valutazione finora
- Floyd17 TB Ch05Documento5 pagineFloyd17 TB Ch05sdjuknicNessuna valutazione finora
- Speed and Agility Training For TennisDocumento3 pagineSpeed and Agility Training For TennissdjuknicNessuna valutazione finora
- Floyd17 TB Ch05Documento5 pagineFloyd17 TB Ch05sdjuknicNessuna valutazione finora
- Floyd17 TB Ch03Documento5 pagineFloyd17 TB Ch03sdjuknicNessuna valutazione finora
- Floyd17 TB Ch08Documento5 pagineFloyd17 TB Ch08sdjuknicNessuna valutazione finora
- Exercise Programs For ChildrenDocumento20 pagineExercise Programs For ChildrensdjuknicNessuna valutazione finora
- Floyd17 TB Ch11Documento5 pagineFloyd17 TB Ch11sdjuknicNessuna valutazione finora
- Total Body CompDocumento13 pagineTotal Body CompsdjuknicNessuna valutazione finora
- The Effect of Backward Walking Treadmill Training On Kinematics of The Trunk and Lower LimbsDocumento7 pagineThe Effect of Backward Walking Treadmill Training On Kinematics of The Trunk and Lower LimbssdjuknicNessuna valutazione finora
- The Operant of TensioDocumento23 pagineThe Operant of TensiosdjuknicNessuna valutazione finora
- The Significance of The J-Curve in Hypertension and PDFDocumento5 pagineThe Significance of The J-Curve in Hypertension and PDFsdjuknicNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Concrete Mixer Rear Discharge Parts Catalog PDFDocumento215 pagineConcrete Mixer Rear Discharge Parts Catalog PDFtecnomaqvl04 tecnomaqNessuna valutazione finora
- Chapter 21 Muscle Blood FlowDocumento17 pagineChapter 21 Muscle Blood Flowelmedina omeragicNessuna valutazione finora
- Collegeresume Monica DifatoDocumento3 pagineCollegeresume Monica Difatoapi-255587712Nessuna valutazione finora
- IELTS Placement Test PDFDocumento11 pagineIELTS Placement Test PDFTamaraKoranjić67% (3)
- YogasanasDocumento25 pagineYogasanaschandrasekharch06Nessuna valutazione finora
- NSK Ball Screws CatalogueDocumento65 pagineNSK Ball Screws Cataloguechidambaram kasiNessuna valutazione finora
- 7 Gray Cook & Stuart McGill Assessing Movement Q&A and Closing Remarks TranscriptDocumento20 pagine7 Gray Cook & Stuart McGill Assessing Movement Q&A and Closing Remarks TranscriptSeba Millón CampañaNessuna valutazione finora
- Conan CCG - Core Set RulesDocumento12 pagineConan CCG - Core Set RulesmrtibblesNessuna valutazione finora
- Bailer 4Documento1 paginaBailer 4samanNessuna valutazione finora
- Trekking Cuzco1Documento3 pagineTrekking Cuzco1Josue John Jaime CardenasNessuna valutazione finora
- Liverpool FC Programmes - Vs Crystal Palace - 18 September 2021Documento86 pagineLiverpool FC Programmes - Vs Crystal Palace - 18 September 2021Gameplay RolixNessuna valutazione finora
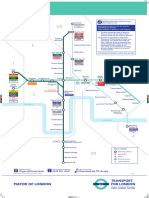
- DLR Route MapDocumento1 paginaDLR Route MapChristopher HollowayNessuna valutazione finora
- Arjun Appadurai, Playing With ModernityDocumento26 pagineArjun Appadurai, Playing With ModernityDhrti SharmaNessuna valutazione finora
- CC Rules EngDocumento21 pagineCC Rules EngLuciano PanzaNessuna valutazione finora
- AbbaDocumento3 pagineAbbaMina CesarNessuna valutazione finora
- Fileshare CcsDocumento15 pagineFileshare CcssoasklasdjNessuna valutazione finora
- D9 P.B PDFDocumento885 pagineD9 P.B PDFDe Javu100% (1)
- Chapter1 12Documento177 pagineChapter1 12Robertus Hajai0% (1)
- Suzuki Apv Repair Manual: Read/DownloadDocumento2 pagineSuzuki Apv Repair Manual: Read/DownloadPm auto service25% (4)
- Suspension and AxleDocumento100 pagineSuspension and AxleChristian Linares AbreuNessuna valutazione finora
- NFL 101 - Introducing The Basics of Cover 4 - Bleacher ReportDocumento11 pagineNFL 101 - Introducing The Basics of Cover 4 - Bleacher Reportwill27ns100% (1)
- 2011 Nissan Pathfinder Service Repair Manual PDFDocumento16 pagine2011 Nissan Pathfinder Service Repair Manual PDFfjjsjekdmme0% (3)
- POLAR FavorDocumento10 paginePOLAR FavornetsheldonNessuna valutazione finora
- David GogginsDocumento2 pagineDavid GogginsKaotiix0% (1)
- Shaiya Second CommandDocumento4 pagineShaiya Second CommandGuilherme RochaNessuna valutazione finora
- Ajuste Calibracion de Valvulas TH460Documento4 pagineAjuste Calibracion de Valvulas TH460UilmerKrdenasNessuna valutazione finora
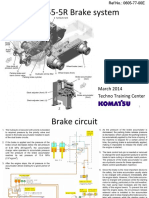
- GD755-5R 06 Brake SystemDocumento22 pagineGD755-5R 06 Brake Systemyongki fcNessuna valutazione finora
- Toledo Mud Hens 2024 ScheduleDocumento1 paginaToledo Mud Hens 2024 ScheduleJake PietraszNessuna valutazione finora
- Module in VolleyballDocumento12 pagineModule in VolleyballAngelica Justo100% (1)
- PoopDocumento4 paginePoopchloeingle23Nessuna valutazione finora