Potrebbero piacerti anche
- Pregnancy HypertensionDocumento30 paginePregnancy HypertensionJon Gab PaquitNessuna valutazione finora
- Fraktur NCP Surgery PDFDocumento4 pagineFraktur NCP Surgery PDFMuklis Al Fadlika100% (1)
- Assessment Nursing Diagnosis Scientific Basis Planning Interventions RationaleDocumento3 pagineAssessment Nursing Diagnosis Scientific Basis Planning Interventions RationaleJose Rey BuenavistaNessuna valutazione finora
- Ectopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Documento10 pagineEctopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNessuna valutazione finora
- Role Nurse Exec Patient SafetyDocumento4 pagineRole Nurse Exec Patient SafetyInesNessuna valutazione finora
- Bed SoreDocumento10 pagineBed Soreanon-190359Nessuna valutazione finora
- Increasing Early and Exclusive Breastfeeding in Rural Uttar PradeshDocumento8 pagineIncreasing Early and Exclusive Breastfeeding in Rural Uttar Pradeshtika tikaNessuna valutazione finora
- Ladybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPDocumento2 pagineLadybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPLadybelle GototosNessuna valutazione finora
- Feliciano, Troy Ivan Silva, Queenie Rose V. BSN 3-C: Rationale: To Track The Changes of Client's ConditionDocumento4 pagineFeliciano, Troy Ivan Silva, Queenie Rose V. BSN 3-C: Rationale: To Track The Changes of Client's ConditionQueenie SilvaNessuna valutazione finora
- Activity IntoleranceDocumento1 paginaActivity IntoleranceRonlene CoronelNessuna valutazione finora
- "My Breasts Are Sore and Tender But There Is No Milk Coming Out and Im Also in Pain Due To Uterine CrampingDocumento3 pagine"My Breasts Are Sore and Tender But There Is No Milk Coming Out and Im Also in Pain Due To Uterine CrampingBAGUIO CATSNessuna valutazione finora
- CTG Booklet: A Quick Reference Guide For Managing CtgsDocumento16 pagineCTG Booklet: A Quick Reference Guide For Managing Ctgscirlce:twoworldsconnectedNessuna valutazione finora
- HERNIADocumento27 pagineHERNIAVanessa SumalbagNessuna valutazione finora
- Beta ThalaDocumento2 pagineBeta ThalaAngie LamoNessuna valutazione finora
- II. General and Specific ObjectivesDocumento5 pagineII. General and Specific ObjectivesRae Marie AquinoNessuna valutazione finora
- Essential Intrapartum and Newborn Care 1Documento5 pagineEssential Intrapartum and Newborn Care 1Genierose YantoNessuna valutazione finora
- Premature LaborDocumento59 paginePremature LaborAmiel Francisco ReyesNessuna valutazione finora
- 68 Abnormal PeuperiumDocumento44 pagine68 Abnormal PeuperiumGodsonYeboah-AwudziNessuna valutazione finora
- NCP Cavernous Sinus ThrombosisDocumento3 pagineNCP Cavernous Sinus ThrombosisVencel Mae Famas Villahermosa50% (2)
- Seizure Care PLNDocumento9 pagineSeizure Care PLNAkhil Paul Kuriakose ManalelNessuna valutazione finora
- Nursing Care Plan of The NewbornDocumento4 pagineNursing Care Plan of The Newbornbowki namoNessuna valutazione finora
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocumento7 pagineHANDOUT Chapter 11 Promoting Fetal and Maternal HealthClouiseNessuna valutazione finora
- College of NursingDocumento54 pagineCollege of NursingJan VillaminNessuna valutazione finora
- Health Talk Om Antenatal ExerciseDocumento10 pagineHealth Talk Om Antenatal ExerciseDeepika PatidarNessuna valutazione finora
- VVF Clinical Presentation 1Documento24 pagineVVF Clinical Presentation 1georgeloto12Nessuna valutazione finora
- Assessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataDocumento2 pagineAssessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataJoan GuisicNessuna valutazione finora
- MastitisDocumento13 pagineMastitisapi-232713902Nessuna valutazione finora
- Post Operative Care After AmputationDocumento11 paginePost Operative Care After AmputationEka MahayundhariNessuna valutazione finora
- 05 DystociaDocumento10 pagine05 DystociaRiantiara PutrizaNessuna valutazione finora
- ماتيرنتي NcpDocumento3 pagineماتيرنتي Ncpلمى الشهريNessuna valutazione finora
- 5 BubbleheDocumento1 pagina5 BubbleheErick SumicadNessuna valutazione finora
- Nursing Care PlanDocumento6 pagineNursing Care PlanJohann OrtizNessuna valutazione finora
- Active Management of Normal LabourDocumento16 pagineActive Management of Normal LabourjincyneeleshNessuna valutazione finora
- "Nilalagnat Ang Anak Ko." AsDocumento2 pagine"Nilalagnat Ang Anak Ko." AsgeorgiaNessuna valutazione finora
- Care Plan PedsDocumento7 pagineCare Plan PedsdjbhetaNessuna valutazione finora
- NCP Draft - Ectopic PregnancyDocumento7 pagineNCP Draft - Ectopic PregnancyD CNessuna valutazione finora
- Episiotomy Wound Haematoma: Recognition, Management and Healing Assessment by REEDA Scale in Postpartum PeriodDocumento4 pagineEpisiotomy Wound Haematoma: Recognition, Management and Healing Assessment by REEDA Scale in Postpartum PeriodIOSRjournalNessuna valutazione finora
- CataractsDocumento37 pagineCataractsIbrahimalpha BadarakamaraNessuna valutazione finora
- Management MastitisDocumento6 pagineManagement MastitisReza Hardian NatsirNessuna valutazione finora
- Gestational Diabetes Mellitus Gestational Diabetes Mellitus (GDM) Is One of TheDocumento10 pagineGestational Diabetes Mellitus Gestational Diabetes Mellitus (GDM) Is One of TheJobelle AcenaNessuna valutazione finora
- Nursing Care Plans: Desired Outcome Interventions Impaired Physical MobilityDocumento6 pagineNursing Care Plans: Desired Outcome Interventions Impaired Physical MobilityNaomi MasudaNessuna valutazione finora
- EvistaDocumento18 pagineEvistaBrankoPopovićNessuna valutazione finora
- Gestational Thropoblastic DiseaseDocumento56 pagineGestational Thropoblastic DiseaseGringo Barroga0% (1)
- Neonatal PneumoniaDocumento1 paginaNeonatal PneumoniaAlyssa Rose MacasiebNessuna valutazione finora
- Operative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Documento71 pagineOperative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Jhon Negesse100% (1)
- EndometriosisDocumento6 pagineEndometriosissalamredNessuna valutazione finora
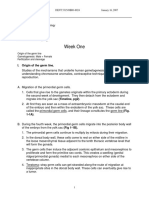
- Week One: I. Origin of The Germ LineDocumento67 pagineWeek One: I. Origin of The Germ LinerohitNessuna valutazione finora
- NCP - Impaired Gas Exchange (COPD)Documento3 pagineNCP - Impaired Gas Exchange (COPD)Karen Joy ItoNessuna valutazione finora
- Chronic Obstructive Pulmonary Disease Bronchitis Nursing Care PlansDocumento10 pagineChronic Obstructive Pulmonary Disease Bronchitis Nursing Care Planscy belNessuna valutazione finora
- Seizure Disorders in ChildrenDocumento22 pagineSeizure Disorders in ChildrenBheru LalNessuna valutazione finora
- NCP-Drug Study 2Documento4 pagineNCP-Drug Study 2hsiriaNessuna valutazione finora
- BMC Transitions of CareDocumento2 pagineBMC Transitions of Carebalab2311Nessuna valutazione finora
- Post PartumDocumento22 paginePost PartumShaira Mae Yante RomeroNessuna valutazione finora
- NCP Knowledge DeficitDocumento2 pagineNCP Knowledge DeficitRainier IbarretaNessuna valutazione finora
- NCP GeDocumento14 pagineNCP GeSuluhTriUtomoNessuna valutazione finora
- Postpartum NCPDocumento20 paginePostpartum NCPireneNessuna valutazione finora
- Antenatal ExaminationDocumento18 pagineAntenatal ExaminationMiu MiuNessuna valutazione finora
- PoliomyelitisDocumento4 paginePoliomyelitisGerard Adad Misa100% (1)
- Antepartal Assessment Rubric With RationaleDocumento6 pagineAntepartal Assessment Rubric With RationaleSupremo Manuel M DeluaoNessuna valutazione finora
- Ielts Vocab - Podcasts NotesDocumento2 pagineIelts Vocab - Podcasts NotesNina MoradaNessuna valutazione finora
- NCLEX Quick Fix III - Sessions 7 To 9 - Handouts PDFDocumento34 pagineNCLEX Quick Fix III - Sessions 7 To 9 - Handouts PDFNina MoradaNessuna valutazione finora
- Course: Leadership and Change ManagementDocumento10 pagineCourse: Leadership and Change ManagementNina MoradaNessuna valutazione finora
- ACLS Study Guide JULY 2021 UPDATEDocumento3 pagineACLS Study Guide JULY 2021 UPDATENina Morada100% (2)
- CSSD - Clean AreaDocumento2 pagineCSSD - Clean AreaNina MoradaNessuna valutazione finora
- Curriculum Vitae FormDocumento2 pagineCurriculum Vitae FormNina MoradaNessuna valutazione finora
- Assessment Item - EssayDocumento1 paginaAssessment Item - EssayNina MoradaNessuna valutazione finora
- HSM-519-Assignment and Evaluation CriteriaDocumento2 pagineHSM-519-Assignment and Evaluation CriteriaNina MoradaNessuna valutazione finora
- NCLEX Quick Fix III - Sessions 7 To 9 - Handouts PDFDocumento34 pagineNCLEX Quick Fix III - Sessions 7 To 9 - Handouts PDFNina MoradaNessuna valutazione finora
- Writing Task 2Documento1 paginaWriting Task 2Nina MoradaNessuna valutazione finora
- Writing Task 1Documento2 pagineWriting Task 1Nina MoradaNessuna valutazione finora
- Musical Theatre Is A Form of Theatrical Performance That Combines SongsDocumento2 pagineMusical Theatre Is A Form of Theatrical Performance That Combines SongsNina MoradaNessuna valutazione finora
- Diagnostic Procedures Final 1Documento4 pagineDiagnostic Procedures Final 1Nina MoradaNessuna valutazione finora
- Case 1 ExampleDocumento26 pagineCase 1 ExampleNina MoradaNessuna valutazione finora
- Affidavit of Support and Consent: Born On inDocumento1 paginaAffidavit of Support and Consent: Born On inNina MoradaNessuna valutazione finora
- Writing Task 1Documento2 pagineWriting Task 1Nina Morada100% (1)
- Banquet MenuDocumento48 pagineBanquet MenuNina MoradaNessuna valutazione finora
- IntroDocumento2 pagineIntroNina MoradaNessuna valutazione finora
- Case 1 ExampleDocumento25 pagineCase 1 ExampleNina MoradaNessuna valutazione finora
- Psychiatric Nursing: Universidad de Sta. Isabel College of NursingDocumento4 paginePsychiatric Nursing: Universidad de Sta. Isabel College of NursingNina MoradaNessuna valutazione finora
- Patient'S Data: Universidad de Sta. Isabel College of Nursing A/Y 2017-2018Documento1 paginaPatient'S Data: Universidad de Sta. Isabel College of Nursing A/Y 2017-2018Nina MoradaNessuna valutazione finora
- High Alert Medication PlanDocumento15 pagineHigh Alert Medication PlanNina Morada100% (5)
- Journal of Atmospheric Science Research - Vol.5, Iss.4 October 2022Documento54 pagineJournal of Atmospheric Science Research - Vol.5, Iss.4 October 2022Bilingual PublishingNessuna valutazione finora
- Britannia Volume 12 Issue 1981 (Doi 10.2307/526240) Michael P. Speidel - Princeps As A Title For 'Ad Hoc' CommandersDocumento8 pagineBritannia Volume 12 Issue 1981 (Doi 10.2307/526240) Michael P. Speidel - Princeps As A Title For 'Ad Hoc' CommandersSteftyraNessuna valutazione finora
- Revit 2023 Architecture FudamentalDocumento52 pagineRevit 2023 Architecture FudamentalTrung Kiên TrầnNessuna valutazione finora
- A Review of Mechanism Used in Laparoscopic Surgical InstrumentsDocumento15 pagineA Review of Mechanism Used in Laparoscopic Surgical InstrumentswafasahilahNessuna valutazione finora
- Bag Technique and Benedict ToolDocumento2 pagineBag Technique and Benedict ToolAriel Delos Reyes100% (1)
- IMC - BisleriDocumento8 pagineIMC - BisleriVineetaNessuna valutazione finora
- Health and Safety For The Meat Industry: Guidance NotesDocumento198 pagineHealth and Safety For The Meat Industry: Guidance NotesPredrag AndjelkovicNessuna valutazione finora
- 200150, 200155 & 200157 Accelerometers: DescriptionDocumento16 pagine200150, 200155 & 200157 Accelerometers: DescriptionJOSE MARIA DANIEL CANALESNessuna valutazione finora
- List of The Legend of Korra Episodes - Wikipedia PDFDocumento27 pagineList of The Legend of Korra Episodes - Wikipedia PDFEmmanuel NocheNessuna valutazione finora
- Report On Marketing Strategy of Nestle MILKPAKDocumento13 pagineReport On Marketing Strategy of Nestle MILKPAKAzeem Ahmad100% (1)
- Elastomeric Impression MaterialsDocumento6 pagineElastomeric Impression MaterialsMarlene CasayuranNessuna valutazione finora
- Eu Schengen Catalogue enDocumento54 pagineEu Schengen Catalogue enSorin din ConstanțaNessuna valutazione finora
- Tree PruningDocumento15 pagineTree Pruningrita44Nessuna valutazione finora
- PreviewpdfDocumento83 paginePreviewpdfJohana GavilanesNessuna valutazione finora
- Ideal Gas Law Lesson Plan FinalDocumento5 pagineIdeal Gas Law Lesson Plan FinalLonel SisonNessuna valutazione finora
- Redirection & PipingDocumento16 pagineRedirection & PipingPraveen PatelNessuna valutazione finora
- P. E. and Health ReportDocumento20 pagineP. E. and Health ReportLESSLY ABRENCILLONessuna valutazione finora
- PDF of Tally ShortcutsDocumento6 paginePDF of Tally ShortcutsSuraj Mehta100% (2)
- Karthik ResumeDocumento2 pagineKarthik ResumeArun Raj ANessuna valutazione finora
- 2 AcknowledgementDocumento8 pagine2 AcknowledgementPadil KonamiNessuna valutazione finora
- Industrial Machine and ControlsDocumento31 pagineIndustrial Machine and ControlsCarol Soi100% (4)
- Geotechnical Aspects of Open Stope Design at BHP Cannington: G C StreetonDocumento7 pagineGeotechnical Aspects of Open Stope Design at BHP Cannington: G C StreetonJuan PerezNessuna valutazione finora
- Docsity Detailed Lesson Plan 5Documento4 pagineDocsity Detailed Lesson Plan 5Sydie MoredoNessuna valutazione finora
- Assignment Csi104Documento11 pagineAssignment Csi104Minh Lê KhảiNessuna valutazione finora
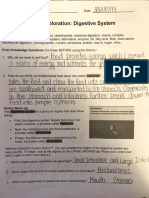
- Student Exploration: Digestive System: Food Inio Simple Nutrien/oDocumento9 pagineStudent Exploration: Digestive System: Food Inio Simple Nutrien/oAshantiNessuna valutazione finora
- Lecture Notes 3A - Basic Concepts of Crystal Structure 2019Documento19 pagineLecture Notes 3A - Basic Concepts of Crystal Structure 2019Lena BacaniNessuna valutazione finora
- DIFFERENTIATING PERFORMANCE TASK FOR DIVERSE LEARNERS (Script)Documento2 pagineDIFFERENTIATING PERFORMANCE TASK FOR DIVERSE LEARNERS (Script)Laurice Carmel AgsoyNessuna valutazione finora
- Process Strategy: Powerpoint Slides by Jeff HeylDocumento13 pagineProcess Strategy: Powerpoint Slides by Jeff HeylMuizzNessuna valutazione finora
- Meniere's Disease - Retinal Detatchment - GlaucomaDocumento3 pagineMeniere's Disease - Retinal Detatchment - Glaucomaybet03Nessuna valutazione finora
- The Grass Rink Summer Final 2019Documento9 pagineThe Grass Rink Summer Final 2019api-241553699Nessuna valutazione finora