Potrebbero piacerti anche
- OSCE Cheat SheetDocumento3 pagineOSCE Cheat SheetazarsamaniNessuna valutazione finora
- Better A Surgeons Notes On PerformanceDocumento2 pagineBetter A Surgeons Notes On PerformanceDivyesh DholariyaNessuna valutazione finora
- Tacfit Warrior ManualDocumento94 pagineTacfit Warrior ManualFlakko13788% (8)
- Gynaecological History Taking - Geeky MedicsDocumento6 pagineGynaecological History Taking - Geeky MedicsMariam Mohamed100% (1)
- General Exam and Q&A For MBBS DR ShamolDocumento320 pagineGeneral Exam and Q&A For MBBS DR Shamolmaybe100% (3)
- CARAS SCUTSHEET 2nd EditDocumento2 pagineCARAS SCUTSHEET 2nd EditFrances Katrina Siruno100% (1)
- MedSisters OSCE NotesDocumento108 pagineMedSisters OSCE NotesAmrita HarrilalNessuna valutazione finora
- Pediatric Clinical ExaminationDocumento3 paginePediatric Clinical ExaminationAlexander EnnesNessuna valutazione finora
- Newborn ExaminationDocumento45 pagineNewborn ExaminationHamka HamNessuna valutazione finora
- Electronic Fetal MonitoringDocumento4 pagineElectronic Fetal MonitoringMauZungNessuna valutazione finora
- DR C BravadoDocumento2 pagineDR C Bravadomtrigott100% (1)
- NSTEMI - PathophysiologyDocumento4 pagineNSTEMI - PathophysiologyDivyesh DholariyaNessuna valutazione finora
- Chicken Embryo Lab ReportDocumento10 pagineChicken Embryo Lab Reportgmk5031Nessuna valutazione finora
- How To Read A CTGDocumento12 pagineHow To Read A CTGRachel Lalaine Marie G. SialanaNessuna valutazione finora
- Paeds Handbook Class2021 1568487638Documento30 paginePaeds Handbook Class2021 1568487638kafosidNessuna valutazione finora
- !THe H Book For 5th Year OSCE - Part 1 PDFDocumento147 pagine!THe H Book For 5th Year OSCE - Part 1 PDFMalvinder Singh DhillonNessuna valutazione finora
- Shoulder Examination Mark SchemeDocumento1 paginaShoulder Examination Mark Schemegus_lionsNessuna valutazione finora
- Mental State Exam OSCE Mark SchemeDocumento2 pagineMental State Exam OSCE Mark SchemeoluseyeNessuna valutazione finora
- Shock PresentationDocumento20 pagineShock Presentationrosalyn sugayNessuna valutazione finora
- How To Read An ECGDocumento21 pagineHow To Read An ECGSlychenkoNessuna valutazione finora
- Newborn NotesDocumento44 pagineNewborn NotesHaziq KamardinNessuna valutazione finora
- Thyroid Status Examination OSCE GuideDocumento20 pagineThyroid Status Examination OSCE GuideemmaNessuna valutazione finora
- OSCE Reviewer 2013Documento4 pagineOSCE Reviewer 2013rere choiNessuna valutazione finora
- Aquifer InternalMedicine09 - 55Documento7 pagineAquifer InternalMedicine09 - 55JulieNessuna valutazione finora
- Mnemonics and Acronyms For Nursing SchoolDocumento20 pagineMnemonics and Acronyms For Nursing SchoolFaye G.100% (3)
- Aquifer InternalMedicine11 - 45Documento8 pagineAquifer InternalMedicine11 - 45JulieNessuna valutazione finora
- Neonatal Jaundice ThresholdsDocumento9 pagineNeonatal Jaundice ThresholdsMariemma TipianiNessuna valutazione finora
- EKGDocumento31 pagineEKGJay JiangNessuna valutazione finora
- Top 93 Nursing SkillsDocumento25 pagineTop 93 Nursing SkillsericNessuna valutazione finora
- Pediatric Notes Draft 12 1Documento98 paginePediatric Notes Draft 12 1Aljon S. TemploNessuna valutazione finora
- Mnemonics PDFDocumento15 pagineMnemonics PDFbeingfiredNessuna valutazione finora
- Reviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixDocumento10 pagineReviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixJamora ManilynNessuna valutazione finora
- Obstetric Abdominal Examination OSCE GuideDocumento16 pagineObstetric Abdominal Examination OSCE GuideMuhammad Aamir IqbalNessuna valutazione finora
- Abdominal Examination - OSCE Guide - Geeky MedicsDocumento9 pagineAbdominal Examination - OSCE Guide - Geeky MedicsJahangir Alam100% (1)
- OBGYN NotesDocumento29 pagineOBGYN NotesavavNessuna valutazione finora
- Cranial Nerve ExaminationDocumento3 pagineCranial Nerve Examinationapi-195986134Nessuna valutazione finora
- Bones of The Foot - Tarsal Bones - Metatarsal Bone - Geeky MedicsDocumento9 pagineBones of The Foot - Tarsal Bones - Metatarsal Bone - Geeky MedicsMohammed ShaikNessuna valutazione finora
- Pediatrics MnemonicsDocumento11 paginePediatrics MnemonicsBitu JaaNessuna valutazione finora
- Cardiovascular BigDocumento37 pagineCardiovascular Bigfaiz nasirNessuna valutazione finora
- BluePrint 5th QuestionsDocumento25 pagineBluePrint 5th QuestionsAbuFreihNessuna valutazione finora
- CVS Nac-Osce BlocksDocumento35 pagineCVS Nac-Osce BlocksRoop SinghNessuna valutazione finora
- OSCE Internal MedicineDocumento4 pagineOSCE Internal Medicinemohamed mowafeyNessuna valutazione finora
- Newborn Assessment ChartDocumento1 paginaNewborn Assessment ChartRupert AsesorNessuna valutazione finora
- Dermpath Cheat SheetDocumento2 pagineDermpath Cheat SheetBob LoblawNessuna valutazione finora
- Medical MnemonicsDocumento15 pagineMedical MnemonicsPrashantVedwanNessuna valutazione finora
- Ecg PDFDocumento70 pagineEcg PDFlauras3005Nessuna valutazione finora
- History & Physical Diagnostic#Documento106 pagineHistory & Physical Diagnostic#Olsa Alshapira100% (1)
- Assesment of The Newborn Baby-KuliahDocumento67 pagineAssesment of The Newborn Baby-Kuliahamel015Nessuna valutazione finora
- Cardiovascular History Taking and Physical ExaminationsDocumento35 pagineCardiovascular History Taking and Physical ExaminationsEndalk AsfawNessuna valutazione finora
- Cheat Sheet (Draft)Documento3 pagineCheat Sheet (Draft)bonziebuddyNessuna valutazione finora
- Hands:, Tablets, Wheelchair, WarfarinDocumento16 pagineHands:, Tablets, Wheelchair, WarfarinRhythm VasudevaNessuna valutazione finora
- Pediatrics NotesDocumento72 paginePediatrics NotesSHEENA MAE DE LOS REYESNessuna valutazione finora
- DR - Majid NotesDocumento16 pagineDR - Majid NotesSandeep Sasidharan100% (1)
- History Taking in PaediatricsDocumento3 pagineHistory Taking in PaediatricsHajar Hanis SofiaNessuna valutazione finora
- Abdominal OSCE Exam ChecklistDocumento3 pagineAbdominal OSCE Exam ChecklistqmajidNessuna valutazione finora
- New Intern Guide Quick NotesDocumento8 pagineNew Intern Guide Quick NotesTrisNessuna valutazione finora
- OB OSCE ReviewerDocumento5 pagineOB OSCE ReviewerPao Ali100% (1)
- I. Inspection: Cardiovascular ExamDocumento136 pagineI. Inspection: Cardiovascular ExamMarbella39Nessuna valutazione finora
- HY Mixed USMLE Review Part I 1Documento20 pagineHY Mixed USMLE Review Part I 1Jennifer Ross-ComptisNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Pathophysiology of Dengue EncephalitisDocumento5 paginePathophysiology of Dengue EncephalitisDivyesh DholariyaNessuna valutazione finora
- Study Guide For International StudentsDocumento35 pagineStudy Guide For International StudentsDivyesh DholariyaNessuna valutazione finora
- Dholariya, Divyesh: Pro: Surviving Sepsis Guidelines 2016Documento8 pagineDholariya, Divyesh: Pro: Surviving Sepsis Guidelines 2016Divyesh DholariyaNessuna valutazione finora
- MAY 07-23-Emf-Filters-For-Electromagnetic-Hypersensitivity PDFDocumento14 pagineMAY 07-23-Emf-Filters-For-Electromagnetic-Hypersensitivity PDFJONATHAN KAPLANNessuna valutazione finora
- Physiological Adaptation of Cardiovascular System To High AltitudeDocumento11 paginePhysiological Adaptation of Cardiovascular System To High AltitudeNicholas Matthew SantosoNessuna valutazione finora
- Thintea Fitness GuideDocumento24 pagineThintea Fitness GuideAmy du PreezNessuna valutazione finora
- VETERINARY NEUROPHARMACOLOGY Practical ManualDocumento40 pagineVETERINARY NEUROPHARMACOLOGY Practical ManualSunil100% (1)
- Electrocardiography II StudentDocumento20 pagineElectrocardiography II StudentArmando Valdez ZamoranoNessuna valutazione finora
- Fix Lab Report 3 (Content) PDFDocumento12 pagineFix Lab Report 3 (Content) PDFLuh RikaNessuna valutazione finora
- 16-Week Harvey Walden MarathonTraining PlanDocumento18 pagine16-Week Harvey Walden MarathonTraining PlanKaren MiranoNessuna valutazione finora
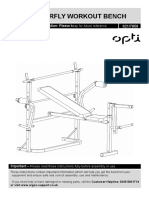
- Opti Butterfly Workout Bench: Assembly & User Instruction 621/7859Documento27 pagineOpti Butterfly Workout Bench: Assembly & User Instruction 621/7859TunaNessuna valutazione finora
- Factors Affecting Pulse RateDocumento2 pagineFactors Affecting Pulse RatetmyliergebunnyNessuna valutazione finora
- Biology Practical 7Documento5 pagineBiology Practical 7robinasanga09Nessuna valutazione finora
- PE1 New Midterm Lesson ProperDocumento44 paginePE1 New Midterm Lesson ProperJesica BalanNessuna valutazione finora
- PSC Issue 30Documento32 paginePSC Issue 30nkosidlaminiNessuna valutazione finora
- The Effect of Cilostazol On Right Heart FunctionDocumento43 pagineThe Effect of Cilostazol On Right Heart FunctionGunawan YogaNessuna valutazione finora
- Harvard Step TestDocumento4 pagineHarvard Step TestKiran ShahidNessuna valutazione finora
- Nur 355 Rotation JournalDocumento3 pagineNur 355 Rotation Journalapi-689882394Nessuna valutazione finora
- Exercise Physio CHP 16 PresentationDocumento10 pagineExercise Physio CHP 16 PresentationSimra ZahidNessuna valutazione finora
- '07 Sullivan CDocumento32 pagine'07 Sullivan CGeo NavarroNessuna valutazione finora
- Training Running Training GuideDocumento23 pagineTraining Running Training GuideCircus StarsiderNessuna valutazione finora
- Exercise DiaryDocumento7 pagineExercise DiaryKristine PunzalanNessuna valutazione finora
- Aruba-Coaching 21st Century (Kompatibilitätsmodus)Documento44 pagineAruba-Coaching 21st Century (Kompatibilitätsmodus)craig1014Nessuna valutazione finora
- What Type of Resistance Training Program Can Help Increase Muscle MassDocumento75 pagineWhat Type of Resistance Training Program Can Help Increase Muscle Massyokimura dimaunahanNessuna valutazione finora
- Vista 120 S Patient Monitoring Solution: 305 MM (12") TFT Color Touchscreen Medibus/Medubus-X ConnectivityDocumento14 pagineVista 120 S Patient Monitoring Solution: 305 MM (12") TFT Color Touchscreen Medibus/Medubus-X ConnectivitydiegolimanaNessuna valutazione finora
- PHED 11n Midterm Reviewer FinalDocumento5 paginePHED 11n Midterm Reviewer FinalGrace Ann E. BulanNessuna valutazione finora
- 5 Step System Stronger Cycling RCADocumento23 pagine5 Step System Stronger Cycling RCAZoran DjordjevicNessuna valutazione finora
- Activity IntoleranceDocumento3 pagineActivity IntoleranceKian Justin HidalgoNessuna valutazione finora
- The Fastest Way To Your Next Personal Best 06-18-21Documento67 pagineThe Fastest Way To Your Next Personal Best 06-18-21Domagoj KušanićNessuna valutazione finora
- Biology Lab Homeostasis and ExerciseDocumento4 pagineBiology Lab Homeostasis and ExerciseCamille GayleNessuna valutazione finora
- Arduino Based Heart Rate Monitor ProjectDocumento7 pagineArduino Based Heart Rate Monitor ProjectMaged Alqubati100% (1)