Potrebbero piacerti anche
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocumento3 pagineVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657Nessuna valutazione finora
- Chest Pain Notes USMLE Step 3Documento3 pagineChest Pain Notes USMLE Step 3kisria100% (1)
- Rhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Documento10 pagineRhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Luis PadillaNessuna valutazione finora
- St-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielDocumento28 pagineSt-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielLloyd Daniel BarrantesNessuna valutazione finora
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocumento6 pagineAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNessuna valutazione finora
- Clinical Learning Session-Acute Coronary Syndromes Acs - 1Documento31 pagineClinical Learning Session-Acute Coronary Syndromes Acs - 1api-611918048Nessuna valutazione finora
- Cme Acs 2. Stemi (Izzah)Documento36 pagineCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNessuna valutazione finora
- Acute Coronary Syndromes - HandoutDocumento4 pagineAcute Coronary Syndromes - Handoutapi-641524095Nessuna valutazione finora
- Sample Case ScenarioDocumento8 pagineSample Case ScenarioJan Crizza Dale R. FrancoNessuna valutazione finora
- Arrhythmias EmergencyDocumento10 pagineArrhythmias EmergencyNITACORDEIRONessuna valutazione finora
- Acute Stroke ProtocolDocumento3 pagineAcute Stroke ProtocolKarissaNessuna valutazione finora
- Tatalaksana ArrthytmiaDocumento55 pagineTatalaksana ArrthytmiaJanstine FirstiandyNessuna valutazione finora
- Acs CCS 2021 KLDocumento52 pagineAcs CCS 2021 KLPitchya WangmeesriNessuna valutazione finora
- Treatment Protocol of SnakebiteDocumento23 pagineTreatment Protocol of SnakebiteEduconsultNessuna valutazione finora
- Pre EclampsiaDocumento9 paginePre EclampsiaAnixa GutiérrezNessuna valutazione finora
- ACS ChartDocumento1 paginaACS ChartJoey TingNessuna valutazione finora
- Acute Coronary SyndromesDocumento7 pagineAcute Coronary SyndromesOwen J. WieseNessuna valutazione finora
- TPA Protocol: Stroke in Carefully Selected PersonsDocumento4 pagineTPA Protocol: Stroke in Carefully Selected PersonsJavier Gonzalez, M.D. DABEMNessuna valutazione finora
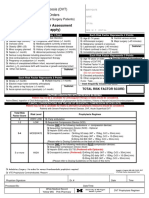
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocumento2 pagineThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNessuna valutazione finora
- OSCE EmergencyDocumento26 pagineOSCE EmergencyXu PeihaoNessuna valutazione finora
- CardiovascularDocumento23 pagineCardiovascularzacks nyirongoNessuna valutazione finora
- Crisis of Hypertension Revised 1Documento57 pagineCrisis of Hypertension Revised 1keenmunir100% (4)
- ParulDocumento7 pagineParulПарул КатіярNessuna valutazione finora
- ACLS ACS Algorithm NewDocumento3 pagineACLS ACS Algorithm Newsambo100% (1)
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Documento9 pagineO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNessuna valutazione finora
- TachycardiaDocumento7 pagineTachycardiaArvind SahniNessuna valutazione finora
- NSTEMI Management: MHAM-College of MedicineDocumento14 pagineNSTEMI Management: MHAM-College of MedicineMykki Gigi NateNessuna valutazione finora
- Acute Coronary SyndromeDocumento5 pagineAcute Coronary Syndromem3d1k100% (1)
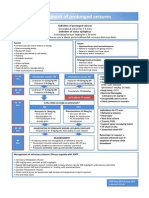
- Treatment of Prolonged SeizuresDocumento1 paginaTreatment of Prolonged SeizuresAhmad ShukriNessuna valutazione finora
- Kegawatan Jantung - MeDocumento41 pagineKegawatan Jantung - MeNam Min BinNessuna valutazione finora
- Tatalaksana STEMI: Rizky Ramadhan N, DR RS Jampang KulonDocumento17 pagineTatalaksana STEMI: Rizky Ramadhan N, DR RS Jampang KulonRizky Ramadhan NuriaNessuna valutazione finora
- AcsDocumento20 pagineAcsTitanSeptiansyahNessuna valutazione finora
- The PatientDocumento9 pagineThe PatientJan Crizza Dale R. FrancoNessuna valutazione finora
- Nstemi 3MBDocumento69 pagineNstemi 3MBDNessuna valutazione finora
- Thrombolytic TherapyDocumento16 pagineThrombolytic TherapyAnonymous nrZXFwNessuna valutazione finora
- Myocardial InfarctionDocumento39 pagineMyocardial InfarctionYauffa Hanna Elt MisykahNessuna valutazione finora
- Supraventricular TachycardiaDocumento7 pagineSupraventricular Tachycardiaagarrido2Nessuna valutazione finora
- Acute Myocardial InfarctionDocumento13 pagineAcute Myocardial InfarctionSajjad KabirNessuna valutazione finora
- Thrombolysis Version 2 0 2015 Final PDFDocumento16 pagineThrombolysis Version 2 0 2015 Final PDFtitisNessuna valutazione finora
- Symptom Onset Arrival: Circle Yes, No or Not Known As AppropriateDocumento2 pagineSymptom Onset Arrival: Circle Yes, No or Not Known As AppropriateB-win IrawanNessuna valutazione finora
- Fac Thrombolysis 2007Documento36 pagineFac Thrombolysis 2007Tri Harjono0% (1)
- Traumatic Brain Injury 2023Documento17 pagineTraumatic Brain Injury 2023Fernando Martinez AguilarNessuna valutazione finora
- Acute Coronary Syndrome Acute MIDocumento41 pagineAcute Coronary Syndrome Acute MIAmjad SobehNessuna valutazione finora
- 11-Acs2 StemiDocumento33 pagine11-Acs2 Stemiمحمد بن الصادقNessuna valutazione finora
- ACLS Simulation ScenariosDocumento14 pagineACLS Simulation ScenariosVanessa HermioneNessuna valutazione finora
- Perfusion, Class 11 ReviewedDocumento45 paginePerfusion, Class 11 ReviewedMelissa GPNessuna valutazione finora
- ACLS Algorithms Adult 2010 Revised May 31 2011Documento12 pagineACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614Nessuna valutazione finora
- Cardiology SBIM Part 1Documento14 pagineCardiology SBIM Part 1Gousay AlkhazmariNessuna valutazione finora
- Strokes Student HandoutDocumento4 pagineStrokes Student HandoutMiss LindiweNessuna valutazione finora
- Treatment Protocol of Snake Bite: Kaushik.H.M 080201388Documento23 pagineTreatment Protocol of Snake Bite: Kaushik.H.M 080201388tiruchanurNessuna valutazione finora
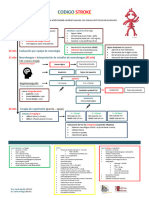
- Codigo Stroke 2Documento1 paginaCodigo Stroke 2Gabriela RuizNessuna valutazione finora
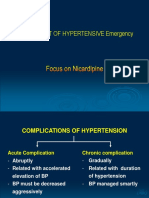
- Management of Hypertensive EmergencyDocumento35 pagineManagement of Hypertensive EmergencyRaditya Indah TofaniNessuna valutazione finora
- Pemicu 6 KGD DeniseDocumento95 paginePemicu 6 KGD DeniseVincent VandestyoNessuna valutazione finora
- STEMI NotesDocumento8 pagineSTEMI NotesIzzul HafiyNessuna valutazione finora
- Acute Myocardial Infarction: Recognition and AssessmentDocumento7 pagineAcute Myocardial Infarction: Recognition and AssessmentHasnainKhimjiNessuna valutazione finora
- Critical Care Drugs 2Documento23 pagineCritical Care Drugs 2Asri Ernadi100% (1)
- Anticoagulation Protocol For PostDocumento8 pagineAnticoagulation Protocol For PostMohammed IbrahimNessuna valutazione finora
- ECG Changes in Drug and Electrolyte AbnormalitiesDocumento28 pagineECG Changes in Drug and Electrolyte AbnormalitiesNachiket Vijay PotdarNessuna valutazione finora
- BLS AlgorithmDocumento9 pagineBLS AlgorithmDr VJ GeorgeNessuna valutazione finora
- NARAYANADocumento19 pagineNARAYANARuchi_Gupta_7482100% (2)
- Beurer BC 08 Blood Pressure MonitorDocumento76 pagineBeurer BC 08 Blood Pressure MonitormihaiylaNessuna valutazione finora
- Supraventrikular & Ventrikular ArrhytmiaDocumento65 pagineSupraventrikular & Ventrikular ArrhytmiarosyadNessuna valutazione finora
- Acls - MegacodeDocumento11 pagineAcls - MegacodeEllen Joyce FlorNessuna valutazione finora
- NCM 118 - Lesson 9 (Heart Failure)Documento6 pagineNCM 118 - Lesson 9 (Heart Failure)Bobby Christian DuronNessuna valutazione finora
- Compensatory Mechanism of Circulatory ShockDocumento29 pagineCompensatory Mechanism of Circulatory ShockWan Razin Wan Hassan100% (1)
- Poster Wecoc PDFDocumento1 paginaPoster Wecoc PDFdikaNessuna valutazione finora
- Hipertensi: Dr. Cici Ariesta Sari UPTD Puskesmas XIII Koto Kampar IDocumento25 pagineHipertensi: Dr. Cici Ariesta Sari UPTD Puskesmas XIII Koto Kampar ICici AriestaNessuna valutazione finora
- ECG Interpretation ECG Interpretation Basics & Quick Guide PDFDocumento157 pagineECG Interpretation ECG Interpretation Basics & Quick Guide PDFNers SenNessuna valutazione finora
- Ebook Electrocardiography For Healthcare Professionals PDF Full Chapter PDFDocumento67 pagineEbook Electrocardiography For Healthcare Professionals PDF Full Chapter PDFkenneth.bell482100% (28)
- Sp088influence of Telmisartan and Amlodipine Combi PDFDocumento3 pagineSp088influence of Telmisartan and Amlodipine Combi PDFKumarsai DurusojuNessuna valutazione finora
- CAD - Ischemic Heart Disease: AtherosclerosisDocumento5 pagineCAD - Ischemic Heart Disease: Atherosclerosisbri ngNessuna valutazione finora
- Alteplase: Umair - M030 Farrakh - M036Documento30 pagineAlteplase: Umair - M030 Farrakh - M036Farrakh AliNessuna valutazione finora
- Micu Case Study d1Documento28 pagineMicu Case Study d1jmarc_2180% (5)
- Roumanian Journal of Cardiology 2018 PDFDocumento418 pagineRoumanian Journal of Cardiology 2018 PDFmiha_virgNessuna valutazione finora
- 1.2.1 Cardio History Taking and Physical Examination Part 1Documento53 pagine1.2.1 Cardio History Taking and Physical Examination Part 1Abanoub AwadallaNessuna valutazione finora
- Administering Metoprolol IV Push 1Documento22 pagineAdministering Metoprolol IV Push 1api-357388170Nessuna valutazione finora
- Charles B. Higgins, Albert de Roos MRI and CT of The Cardiovascular SystemDocumento180 pagineCharles B. Higgins, Albert de Roos MRI and CT of The Cardiovascular SystemdrAlbertoVVNessuna valutazione finora
- Intradialytic Hypertension Time To Act 10Documento7 pagineIntradialytic Hypertension Time To Act 10Nia FirdiantyNessuna valutazione finora
- ACLS Algorithms SlideDocumento26 pagineACLS Algorithms SlidehrsoNessuna valutazione finora
- Atrial Fibrillation - Geeky MedicsDocumento10 pagineAtrial Fibrillation - Geeky MedicsJahangir AlamNessuna valutazione finora
- Essential Paediatrics Course Book 2023Documento88 pagineEssential Paediatrics Course Book 2023alextkijiji_81403773Nessuna valutazione finora
- Coxa Plana PathophysiologyDocumento1 paginaCoxa Plana Pathophysiologymiss RN100% (4)
- Diagram Human Heart Kel 1Documento3 pagineDiagram Human Heart Kel 1Rahma SafitriNessuna valutazione finora
- Singkatan Diagnosa A-ZDocumento23 pagineSingkatan Diagnosa A-ZElisabeth AnitaNessuna valutazione finora
- Salinas2003 PDFDocumento15 pagineSalinas2003 PDFnatashiaNessuna valutazione finora
- Farm TocliDocumento3 pagineFarm TocliPankaj MaithaniNessuna valutazione finora
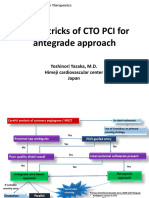
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocumento21 pagineTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNessuna valutazione finora