Potrebbero piacerti anche
- Maxillofacial TraumaDocumento56 pagineMaxillofacial TraumaErnesto Fer FdezNessuna valutazione finora
- Deep Venous ThrombosisDocumento56 pagineDeep Venous ThrombosisSrikant Konchada100% (1)
- Diabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Documento28 pagineDiabetic Foot Ulcer - Yandriyane Stephanie Robiady - 131621190504Yohelio Priawan SibuNessuna valutazione finora
- Deep Vein Thrombosis: Dr. Iman Haryana SPJPDocumento29 pagineDeep Vein Thrombosis: Dr. Iman Haryana SPJPAuliyah SeptianiNessuna valutazione finora
- Rheumatic Heart Disease and Infective EndocarditisDocumento10 pagineRheumatic Heart Disease and Infective Endocarditisapi-19840404Nessuna valutazione finora
- Surgery Lectures EsophagusDocumento22 pagineSurgery Lectures Esophagusj,007Nessuna valutazione finora
- Venous Thrombo Embolism: DR Shams RehanDocumento50 pagineVenous Thrombo Embolism: DR Shams RehanShams RehanNessuna valutazione finora
- Diseases of The Veins: Dr. Pisake Boontham M.D., Ph.D. Department of Surgery Phramongkutklao HospitalDocumento78 pagineDiseases of The Veins: Dr. Pisake Boontham M.D., Ph.D. Department of Surgery Phramongkutklao HospitalgetnusNessuna valutazione finora
- Venous DiseaseDocumento45 pagineVenous DiseaseNinch Nagac100% (1)
- Acute Compartment Syndrome of The ForearmDocumento4 pagineAcute Compartment Syndrome of The ForearmsalamsibiuNessuna valutazione finora
- Colorectal CancerDocumento29 pagineColorectal CancerLeeyanBhadzzVagayNessuna valutazione finora
- My Ideal Home: Name No. Class Date Mark TeacherDocumento5 pagineMy Ideal Home: Name No. Class Date Mark TeacherQuadrado MágicoNessuna valutazione finora
- Fat EmbolismDocumento12 pagineFat EmbolismHastina HadnanNessuna valutazione finora
- Endovenous Laser Treatment of Varicose Veins EVLTDocumento18 pagineEndovenous Laser Treatment of Varicose Veins EVLTCTAFDocuments100% (1)
- Msds EthanolDocumento7 pagineMsds EthanolHeru HarnadiNessuna valutazione finora
- Neoplastic DisordersDocumento36 pagineNeoplastic DisordersJSeasharkNessuna valutazione finora
- Deep Vein ThrombosisDocumento38 pagineDeep Vein ThrombosisvincentthedyNessuna valutazione finora
- Viral Warts (Verrucae) : College of Medicine Name: Qasim Hussain AL-Haleimi AC:207002113Documento18 pagineViral Warts (Verrucae) : College of Medicine Name: Qasim Hussain AL-Haleimi AC:207002113Qasim HaleimiNessuna valutazione finora
- Burn WoundDocumento68 pagineBurn WoundjrefkyNessuna valutazione finora
- Bouncing BallDocumento5 pagineBouncing Ballyamamoto1070% (10)
- PSORIASISDocumento27 paginePSORIASISnurulzakinahnunu100% (1)
- Sclerotherapy Information and Consent FormDocumento3 pagineSclerotherapy Information and Consent FormDaniel DePrince IIINessuna valutazione finora
- Diabetic FootDocumento68 pagineDiabetic FootEndro Ri WibowoNessuna valutazione finora
- Vein Treatment Center - Common Vein Disorders, Telangiectasia, Reticular Vein, Varicose Vein, Corona Phlebectatica, Edema, Hyperpigmentation, Stasis Dermatitis, Lipodermatosclerosis, Atrophie Blanche, Venous Stasis UlcerDocumento14 pagineVein Treatment Center - Common Vein Disorders, Telangiectasia, Reticular Vein, Varicose Vein, Corona Phlebectatica, Edema, Hyperpigmentation, Stasis Dermatitis, Lipodermatosclerosis, Atrophie Blanche, Venous Stasis UlcerPankaj Shrotriya100% (1)
- IKD6 - Contrast Associated AKIDocumento44 pagineIKD6 - Contrast Associated AKIRenal Association MauritiusNessuna valutazione finora
- Zeolites and Ordered Porous Solids - Fundamentals and ApplicationsDocumento376 pagineZeolites and Ordered Porous Solids - Fundamentals and ApplicationsHenrique Souza100% (1)
- Mini AbdominoplastyDocumento4 pagineMini AbdominoplastyAhmad Arbi AninditoNessuna valutazione finora
- Vascular Disease Approach 11-7-13Documento65 pagineVascular Disease Approach 11-7-13Dian PuspaNessuna valutazione finora
- Deep Vein ThrombosisDocumento43 pagineDeep Vein Thrombosisoctaviana_simbolonNessuna valutazione finora
- EpendymomaDocumento5 pagineEpendymomaDenny's BerciaNessuna valutazione finora
- Structural Fat GraftingDocumento19 pagineStructural Fat GraftingGautam KalraNessuna valutazione finora
- Urethral InjuryDocumento56 pagineUrethral InjuryParty NoriNessuna valutazione finora
- Garcia, Melegrito, Zamuco: Perforated Peptic Ulcer DiseaseDocumento4 pagineGarcia, Melegrito, Zamuco: Perforated Peptic Ulcer DiseasePaulo GarciaNessuna valutazione finora
- Examination of Peripheral Vascular Disease and GangreneDocumento33 pagineExamination of Peripheral Vascular Disease and GangrenedrrajeshpsmsNessuna valutazione finora
- Pathophysiology: Rectal CarcinomaDocumento25 paginePathophysiology: Rectal CarcinomaCristina CristinaNessuna valutazione finora
- Postoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDocumento17 paginePostoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDesak PramestiNessuna valutazione finora
- Carcinoma of Lung LectureDocumento37 pagineCarcinoma of Lung Lecturesadaf12345678Nessuna valutazione finora
- Amputation in Lower LimbsDocumento35 pagineAmputation in Lower LimbsSamNessuna valutazione finora
- Classification and Diagnosis of Endometrial HyperplasiaDocumento7 pagineClassification and Diagnosis of Endometrial HyperplasiaaksinuNessuna valutazione finora
- Skin Cancer!Documento8 pagineSkin Cancer!HudiansyahNessuna valutazione finora
- Skin CancerDocumento5 pagineSkin CancerEl FaroukNessuna valutazione finora
- Presentasi Kasus Acne VulgarisDocumento27 paginePresentasi Kasus Acne VulgarisAndi Rizki TenryayuNessuna valutazione finora
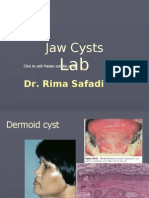
- Lab 4 Jaw Cysts (Slide)Documento80 pagineLab 4 Jaw Cysts (Slide)JustDen09Nessuna valutazione finora
- Wound HealingDocumento17 pagineWound HealingSuci VentasamiaNessuna valutazione finora
- Pages From Grant-Kels - Color Atlas of DermatopathologyDocumento5 paginePages From Grant-Kels - Color Atlas of DermatopathologyamberwinthropNessuna valutazione finora
- IM - Cardiomyopathy and MyocarditisDocumento9 pagineIM - Cardiomyopathy and MyocarditisElisha BernabeNessuna valutazione finora
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDocumento42 pagineChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulNessuna valutazione finora
- Thermal InjuryDocumento35 pagineThermal InjuryIbrahim SalimNessuna valutazione finora
- Approach To The Adult Patient With Anemia - UpToDateDocumento23 pagineApproach To The Adult Patient With Anemia - UpToDateNicole SierraNessuna valutazione finora
- Approach To The Adult With Unexplained Thrombocytopenia - UpToDateDocumento65 pagineApproach To The Adult With Unexplained Thrombocytopenia - UpToDateMagdy GabrNessuna valutazione finora
- 3.mechanical InjuryDocumento127 pagine3.mechanical InjuryARIF-UR-REHMAN100% (2)
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocumento16 pagineDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatevara prasadNessuna valutazione finora
- Carcinoma RectumDocumento28 pagineCarcinoma RectumParul VarshneyNessuna valutazione finora
- OsteoarthritisDocumento15 pagineOsteoarthritisMichael BanksNessuna valutazione finora
- CPM18th Acne VulgarisDocumento9 pagineCPM18th Acne VulgarisMa Katherina ArellanoNessuna valutazione finora
- DiathermyDocumento18 pagineDiathermyrosybashNessuna valutazione finora
- Chylous Fistula of The NeckDocumento44 pagineChylous Fistula of The Neckgk_anandaNessuna valutazione finora
- Vats and Post Op CareDocumento18 pagineVats and Post Op CareVenz100% (1)
- Bone Forming TumorsDocumento81 pagineBone Forming TumorsDoc NaumanNessuna valutazione finora
- ElectrosurgeryDocumento22 pagineElectrosurgeryRavish BangreNessuna valutazione finora
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDocumento57 pagineTumours of The Central Nervous System: FM Brett MD., FrcpathDrGasnasNessuna valutazione finora
- Inguino Scrotal SwellingDocumento3 pagineInguino Scrotal SwellingYurni Dwi AstutiNessuna valutazione finora
- Varicose VeinsDocumento7 pagineVaricose VeinsTarran PhagooNessuna valutazione finora
- Paper 1Documento4 paginePaper 1asa.henfield2Nessuna valutazione finora
- PEPSIDocumento99 paginePEPSIkingloiyaNessuna valutazione finora
- Electrical Inspections: Infrared ThermographyDocumento28 pagineElectrical Inspections: Infrared ThermographyManish RajNessuna valutazione finora
- Feu Sharing Stress MNGTDocumento58 pagineFeu Sharing Stress MNGTsquidsexoNessuna valutazione finora
- Project Final PDFDocumento98 pagineProject Final PDFNgonidzashe MhukaNessuna valutazione finora
- Brochure - Citadines Flatiron Phnom Penh - EnglishDocumento4 pagineBrochure - Citadines Flatiron Phnom Penh - EnglishTix VirakNessuna valutazione finora
- Apti 2Documento17 pagineApti 2Arunkumar MurugappanNessuna valutazione finora
- Civil 416Documento2 pagineCivil 416tskh11Nessuna valutazione finora
- Portable Load Banks: CressallDocumento1 paginaPortable Load Banks: CressallYashveer26Nessuna valutazione finora
- MPDFDocumento5 pagineMPDFRoyalAryansNessuna valutazione finora
- Be Project Presentation SuspensionDocumento17 pagineBe Project Presentation SuspensionGabrielNessuna valutazione finora
- Air Quality Index Analysis & PredictionDocumento34 pagineAir Quality Index Analysis & PredictionGottumukkala Sravan KumarNessuna valutazione finora
- Notes On Peck&Coyle Practical CriticismDocumento10 pagineNotes On Peck&Coyle Practical CriticismLily DameNessuna valutazione finora
- BF02692337 PDFDocumento2 pagineBF02692337 PDFHitesh LokeNessuna valutazione finora
- Nonlinear Analysis and Optimal Design of Reinforced Concrete Plates and ShellsDocumento17 pagineNonlinear Analysis and Optimal Design of Reinforced Concrete Plates and Shellsrodain najjarNessuna valutazione finora
- Marxist Study of The God of Small ThingsDocumento11 pagineMarxist Study of The God of Small ThingsIsrar KhanNessuna valutazione finora
- Lesson Plan 1 - Agriculture in Your LifeDocumento6 pagineLesson Plan 1 - Agriculture in Your Lifeapi-235918896Nessuna valutazione finora
- Haldiram-A Success Story in Family Business: Credit Seminar OnDocumento12 pagineHaldiram-A Success Story in Family Business: Credit Seminar OnAnuNessuna valutazione finora
- Line CodingDocumento27 pagineLine CodingshridonNessuna valutazione finora
- "Chapter 9 - Influence Lines For Statically Determinate Structures" in "Structural Analysis" On Manifold @tupressDocumento33 pagine"Chapter 9 - Influence Lines For Statically Determinate Structures" in "Structural Analysis" On Manifold @tupressrpsirNessuna valutazione finora
- List INN 08february2012 PDFDocumento128 pagineList INN 08february2012 PDFMarisaNessuna valutazione finora
- Chapter Two Feasibility Study 2.0 Methods of Producing Ammonium Sulphate, ( (NH) SO)Documento9 pagineChapter Two Feasibility Study 2.0 Methods of Producing Ammonium Sulphate, ( (NH) SO)Adeyoju RebeccaNessuna valutazione finora
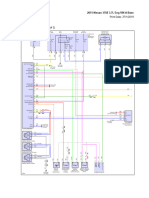
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDocumento69 pagine2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNessuna valutazione finora
- Cengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test BankDocumento26 pagineCengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test Bankladonnaaidanm5s100% (28)
- IoT & WSN - Module 5 - 2018 by Prof - SVDocumento43 pagineIoT & WSN - Module 5 - 2018 by Prof - SVVignesh MJ83% (6)
- HK USP CompactDocumento56 pagineHK USP CompactJonathan CrenshawNessuna valutazione finora