Potrebbero piacerti anche
- CASE REPORT Hip DislocationDocumento42 pagineCASE REPORT Hip DislocationvereriNessuna valutazione finora
- PAD vs. DVTDocumento3 paginePAD vs. DVTKrystel BatinoNessuna valutazione finora
- De Quervain SyndromeDocumento5 pagineDe Quervain SyndromePaula ZorziNessuna valutazione finora
- TractionsDocumento16 pagineTractionsJasmin Jacob100% (1)
- Herniated Nucleus PulposusDocumento38 pagineHerniated Nucleus PulposusAisyah Rieskiu0% (1)
- Supracondylar Humerus FractureDocumento20 pagineSupracondylar Humerus FractureMusyawarah MelalaNessuna valutazione finora
- Coxa PlanaDocumento3 pagineCoxa PlanacarolbeeeNessuna valutazione finora
- Scoliosis PPT B IngDocumento11 pagineScoliosis PPT B IngSyifa Anindya100% (1)
- Herniated Nucleus Pulposus (HNP)Documento14 pagineHerniated Nucleus Pulposus (HNP)CelineNessuna valutazione finora
- Duchenne Muscular DystrophyDocumento3 pagineDuchenne Muscular DystrophyhanzreinherNessuna valutazione finora
- Case Report Epilepsy (English)Documento18 pagineCase Report Epilepsy (English)Ressa OashttamadeaNessuna valutazione finora
- TrH15. Subdural HygromaDocumento3 pagineTrH15. Subdural HygromaRista Nurul Fitria0% (1)
- Spinal Tuberculosis (Pott's Disease)Documento19 pagineSpinal Tuberculosis (Pott's Disease)Komalah ChenasammyNessuna valutazione finora
- Case ReportDocumento38 pagineCase ReportDiLa NandaRiNessuna valutazione finora
- in Growing Toe NailDocumento33 paginein Growing Toe NailEka CresentiaNessuna valutazione finora
- Scoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisDocumento12 pagineScoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisLei Coloma SissonNessuna valutazione finora
- Anatomy of ScoliosisDocumento6 pagineAnatomy of ScoliosisDaniel MañalacNessuna valutazione finora
- Procedural Report Breast Augmentation Drug Study Propofol AnecDocumento15 pagineProcedural Report Breast Augmentation Drug Study Propofol AnecSamer SumalinogNessuna valutazione finora
- Chvostek's Sign and Carpopedal Spasm NEJM APRIL 2009 PDFDocumento1 paginaChvostek's Sign and Carpopedal Spasm NEJM APRIL 2009 PDFAnonymous uVinWXfo4Nessuna valutazione finora
- Fracture of The Femoral NeckDocumento21 pagineFracture of The Femoral NeckSalsabila Al-BasheerNessuna valutazione finora
- # of The Distal RadiusDocumento98 pagine# of The Distal RadiusabhinavaiimsNessuna valutazione finora
- Bilateral Knee OADocumento35 pagineBilateral Knee OAMu'iz Beatforteen50% (2)
- Case Presentation For Blount's Disease B Proximal TibiaDocumento43 pagineCase Presentation For Blount's Disease B Proximal TibiaCzarinah Joyce Novencido0% (1)
- Hip Replacement GuideDocumento28 pagineHip Replacement GuideZulaika NaisNessuna valutazione finora
- Pott's Disease PDFDocumento14 paginePott's Disease PDFRaja RajanNessuna valutazione finora
- Tinea CorporisDocumento23 pagineTinea CorporisDita lewaherillaNessuna valutazione finora
- Congenital Hip DislocationDocumento8 pagineCongenital Hip DislocationSpread MushooNessuna valutazione finora
- Arnold-Chiari Malformations Clinicl Features PDFDocumento3 pagineArnold-Chiari Malformations Clinicl Features PDFsridharNessuna valutazione finora
- Pat 2 Medsurg1Documento20 paginePat 2 Medsurg1api-300849832Nessuna valutazione finora
- OsteomyelitisDocumento47 pagineOsteomyelitisArmand Al HaraaniNessuna valutazione finora
- Cerebrovascular Disease (Emphasis On CVA)Documento29 pagineCerebrovascular Disease (Emphasis On CVA)OlynsieMorrisNessuna valutazione finora
- Tibial FractureDocumento6 pagineTibial FractureKristene June Ilagan CoyamNessuna valutazione finora
- Closed Fracture Tibia FibulaDocumento41 pagineClosed Fracture Tibia FibulaThathmainnul Qulub100% (1)
- Hip Joint DislocationDocumento59 pagineHip Joint DislocationAnonymous P5FDn81yNessuna valutazione finora
- Iontophoresis TENNIS ELBOW (Lateral Humeral Epicondylitis)Documento2 pagineIontophoresis TENNIS ELBOW (Lateral Humeral Epicondylitis)Ikre19Nessuna valutazione finora
- Total Hip ArthroplastyDocumento15 pagineTotal Hip Arthroplastyapi-550438875Nessuna valutazione finora
- Knee DislocationDocumento4 pagineKnee DislocationJohnNessuna valutazione finora
- Herniated Nucleus PulposusDocumento14 pagineHerniated Nucleus PulposusJm Fernandez Gan RNNessuna valutazione finora
- Congenital Talipes Equinovarus (Clubfoot)Documento24 pagineCongenital Talipes Equinovarus (Clubfoot)Boetik AlifiaNessuna valutazione finora
- Acute Appendicitis in ChildrenDocumento71 pagineAcute Appendicitis in ChildrenMohamed KamaraNessuna valutazione finora
- TBWDocumento45 pagineTBWveedee cikalNessuna valutazione finora
- Stump CareDocumento7 pagineStump CareirtazakazmiNessuna valutazione finora
- CTEV - Congenital Club FootDocumento43 pagineCTEV - Congenital Club FootIrfan Ali ShujahNessuna valutazione finora
- Post Burn ContracturesDocumento101 paginePost Burn ContracturesSyed Muhammed Tahir SyedsahibNessuna valutazione finora
- Spinal Cord InjuryDocumento33 pagineSpinal Cord InjuryPriscila Stevanni100% (1)
- Closed Fracture Neck FemurDocumento31 pagineClosed Fracture Neck FemurKiki Said100% (1)
- Referat - JiaDocumento38 pagineReferat - Jiaira danasasmitaNessuna valutazione finora
- Fracture in Leg Tibia and FibulaDocumento27 pagineFracture in Leg Tibia and Fibulachilsya shajiNessuna valutazione finora
- CABGDocumento9 pagineCABGBilal Ali KhanNessuna valutazione finora
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDocumento38 pagineJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalNessuna valutazione finora
- Anterior Cruciate Ligament InjuryDocumento3 pagineAnterior Cruciate Ligament InjuryAdrian Nazario PragachaNessuna valutazione finora
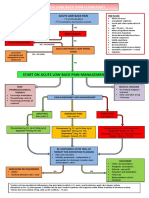
- Acute Low Back Pain Flowchart March 2016Documento1 paginaAcute Low Back Pain Flowchart March 2016Alfiya HasnaNessuna valutazione finora
- Drug StudyDocumento3 pagineDrug StudyNJ CullaNessuna valutazione finora
- 148604-Care Path MENTAL STATUS CHANGE v10 PDFDocumento1 pagina148604-Care Path MENTAL STATUS CHANGE v10 PDFAnonymous 8qVcBze8qNessuna valutazione finora
- Application of Nursing Process To Different Respiratory MedicationsDocumento13 pagineApplication of Nursing Process To Different Respiratory MedicationssharedNessuna valutazione finora
- Headache SummaryDocumento3 pagineHeadache Summaryhameedsabah36Nessuna valutazione finora
- Acute PainDocumento1 paginaAcute Painnursing concept mapsNessuna valutazione finora
- 3C3 Subgroup1 M11 PT1Documento1 pagina3C3 Subgroup1 M11 PT1ENKELI VALDECANTOSNessuna valutazione finora
- Pre Gabal in Drug StudyDocumento1 paginaPre Gabal in Drug StudyHailMarieSBarcenasNessuna valutazione finora
- Fairy Tail - Main ThemeDocumento3 pagineFairy Tail - Main Theme1234chocoNessuna valutazione finora
- Mbs Quick Guide: JULY 2020Documento2 pagineMbs Quick Guide: JULY 20201234chocoNessuna valutazione finora
- Code Geass - StoriesDocumento5 pagineCode Geass - Stories1234chocoNessuna valutazione finora
- Blue BirdDocumento7 pagineBlue Bird1234chocoNessuna valutazione finora
- Doctor Talk: Communication Practice Role PlaysDocumento6 pagineDoctor Talk: Communication Practice Role Plays1234chocoNessuna valutazione finora
- PBM Module1 MTP Template 0Documento2 paginePBM Module1 MTP Template 01234chocoNessuna valutazione finora
- Topical Steroids (Sep 19) PDFDocumento7 pagineTopical Steroids (Sep 19) PDF1234chocoNessuna valutazione finora
- Preoperative AssessmentDocumento9 paginePreoperative Assessment1234chocoNessuna valutazione finora
- Taking A Social and Cultural HistoryDocumento3 pagineTaking A Social and Cultural History1234chocoNessuna valutazione finora
- Managing Mental Illness in Patients From CALD Backgrounds: PsychiatryDocumento5 pagineManaging Mental Illness in Patients From CALD Backgrounds: Psychiatry1234chocoNessuna valutazione finora
- Language of PreventionDocumento9 pagineLanguage of Prevention1234chocoNessuna valutazione finora
- A Conceptual Framework For HealthDocumento1 paginaA Conceptual Framework For Health1234chocoNessuna valutazione finora
- Blue Card Declaration PDFDocumento1 paginaBlue Card Declaration PDF1234chocoNessuna valutazione finora
- Acute Post-Op Pain ManagementDocumento4 pagineAcute Post-Op Pain Management1234chocoNessuna valutazione finora
- Barrett's Esophagus: Identifying The Squamocolumnar (SC) and Gastroesophageal (GE) Junctions EndoscopicallyDocumento10 pagineBarrett's Esophagus: Identifying The Squamocolumnar (SC) and Gastroesophageal (GE) Junctions Endoscopically1234chocoNessuna valutazione finora
- Prenatal Screening Test (AUS) PDFDocumento24 paginePrenatal Screening Test (AUS) PDFshirley_ling_15Nessuna valutazione finora
- Dexamethasone Suppression Tests - VCA Animal HospitalDocumento5 pagineDexamethasone Suppression Tests - VCA Animal HospitaldmantsioNessuna valutazione finora
- Why GILD Remdesivir Is The Only Relevant Coronavirus DrugDocumento8 pagineWhy GILD Remdesivir Is The Only Relevant Coronavirus Drugjulia skripka-serry100% (2)
- IntussusceptionDocumento2 pagineIntussusceptionAireen Mae P. NapigkitNessuna valutazione finora
- Medical Problems and Injuries British English TeacherDocumento5 pagineMedical Problems and Injuries British English TeacherTanitaNessuna valutazione finora
- AAD BF Biopsy TechniquesDocumento2 pagineAAD BF Biopsy TechniquesLos MiNessuna valutazione finora
- Anesthesia For Trauma Patients 05 Apr 2021 ID40Documento10 pagineAnesthesia For Trauma Patients 05 Apr 2021 ID40Erick ToHuNessuna valutazione finora
- LEPTOSPIROSISDocumento14 pagineLEPTOSPIROSISNica Paredes MiravallesNessuna valutazione finora
- Research On Fasting and Cancer TreatmentDocumento9 pagineResearch On Fasting and Cancer TreatmentMNessuna valutazione finora
- Dilatation & Curettage: DR Ayswarya NarayanDocumento19 pagineDilatation & Curettage: DR Ayswarya NarayanPrajwal Kp0% (1)
- Sepsis 23 Dic. 2021Documento2 pagineSepsis 23 Dic. 2021Zonia GuzmanNessuna valutazione finora
- Pamphlet InsideDocumento1 paginaPamphlet Insideapi-2408549370% (1)
- Substance Use Disorders in Children and AdolescentsDocumento21 pagineSubstance Use Disorders in Children and AdolescentsagelvezonNessuna valutazione finora
- Biology Investigatory Project: Samiksha Subhashish SarkarDocumento35 pagineBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarNessuna valutazione finora
- READINGDocumento21 pagineREADINGdiya baby100% (1)
- GlaucomaDocumento15 pagineGlaucomaAmalliaPradisthaNessuna valutazione finora
- Cda Revalida Caregiving NC 2020Documento7 pagineCda Revalida Caregiving NC 2020Rowena Lalongisip De LeonNessuna valutazione finora
- Vats Yustinus Rurie WirawanDocumento6 pagineVats Yustinus Rurie Wirawanrurie wirawanNessuna valutazione finora
- Trisomies: Abnormal Number of ChromosomesDocumento10 pagineTrisomies: Abnormal Number of ChromosomesNaumanNessuna valutazione finora
- 1 Drug Study - DexamethasoneDocumento6 pagine1 Drug Study - DexamethasoneJohn100% (1)
- Delayed Passage of MeconiumDocumento15 pagineDelayed Passage of MeconiumMohammed Ezz El RegalNessuna valutazione finora
- Iron SucroseDocumento3 pagineIron SucroseAtul KumarNessuna valutazione finora
- Mri of Cervical Spine: Location: COLTONDocumento3 pagineMri of Cervical Spine: Location: COLTONSusana FranklinNessuna valutazione finora
- PenileDocumento2 paginePenileAREOLA Vera SophiaNessuna valutazione finora
- Abnormal Psychology Seminar 1Documento1 paginaAbnormal Psychology Seminar 1Daisy RodriguezNessuna valutazione finora
- Aaa Gastrectomy NCP FinalDocumento13 pagineAaa Gastrectomy NCP Finallexzaf100% (1)
- Kapita Selekta Epidemiologi - HO PDFDocumento42 pagineKapita Selekta Epidemiologi - HO PDFDyandri YogiNessuna valutazione finora
- Physical Diagnosis of The ThoraxDocumento3 paginePhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- Urinary Catheter Care Carol RobinsonDocumento34 pagineUrinary Catheter Care Carol RobinsonNihas VayalilNessuna valutazione finora
- GLYBURIDEDocumento3 pagineGLYBURIDEJohn Carlo SamsonNessuna valutazione finora
- Comprehensive Sexuality Education: Developing Responsible Youth Vs Rising RisksDocumento13 pagineComprehensive Sexuality Education: Developing Responsible Youth Vs Rising RisksPatrick Anthony Yongot PadillaNessuna valutazione finora