Potrebbero piacerti anche
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicDa EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicValutazione: 5 su 5 stelle5/5 (1)
- Week 3 Case - DOBDocumento3 pagineWeek 3 Case - DOBKirk Matthew ZhuNessuna valutazione finora
- Rectal CancerDocumento71 pagineRectal CancerGio Balisi100% (2)
- HISTORY # 1 - PCGH, EchavezDocumento11 pagineHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezNessuna valutazione finora
- Discharge Summary JAGONOYDocumento6 pagineDischarge Summary JAGONOYKirstie de LunaNessuna valutazione finora
- Pedia August 29Documento4 paginePedia August 29Raymund AldabaNessuna valutazione finora
- 2 - 23 - 23 AM WardDocumento10 pagine2 - 23 - 23 AM WardkellogskrispiesNessuna valutazione finora
- Cwu SurgeryDocumento16 pagineCwu SurgeryAslah NabilahNessuna valutazione finora
- Case Presentation: Course: EndocrinologyDocumento13 pagineCase Presentation: Course: EndocrinologyCalingalan Hussin CaluangNessuna valutazione finora
- Projectile or Non Projectile?Documento5 pagineProjectile or Non Projectile?Ingrid Ganir GangatNessuna valutazione finora
- Clinical Case: Section A - Group 8Documento68 pagineClinical Case: Section A - Group 8madison Deli100% (1)
- Form Health History Documentation: Biographical DataDocumento7 pagineForm Health History Documentation: Biographical DataSandra SanonNessuna valutazione finora
- Case 3.1Documento11 pagineCase 3.1atdumagNessuna valutazione finora
- Ent Case Report Acute Otitis Media Stage IIIDocumento12 pagineEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- Case 1-PCGH Cerebrovascular DiseaseDocumento40 pagineCase 1-PCGH Cerebrovascular DiseaseHynne Jhea EchavezNessuna valutazione finora
- ADCON April 12 406Documento23 pagineADCON April 12 406Andrassy Twinkle AlineaNessuna valutazione finora
- Case Report VI Internal MedicineDocumento13 pagineCase Report VI Internal MedicineGidu SaidNessuna valutazione finora
- Edited HP I Fri ConfDocumento85 pagineEdited HP I Fri ConfTara Oliveros Dela CruzNessuna valutazione finora
- Chest CaseDocumento19 pagineChest CaseNesma AdelNessuna valutazione finora
- HIVCase Report II Internal MedicineDocumento12 pagineHIVCase Report II Internal Medicineaxmedfare138Nessuna valutazione finora
- Case 4Documento12 pagineCase 4atdumagNessuna valutazione finora
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocumento15 pagineCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNessuna valutazione finora
- Enterobiasis CaseDocumento4 pagineEnterobiasis CaseKimm Delos ReyesNessuna valutazione finora
- Case 2Documento12 pagineCase 2atdumagNessuna valutazione finora
- Pedia 1Documento8 paginePedia 1Jani MisterioNessuna valutazione finora
- Patient History Amang 2Documento7 paginePatient History Amang 2Christine Evan HoNessuna valutazione finora
- Case Report II Internal MedicineDocumento11 pagineCase Report II Internal MedicineGidu SaidNessuna valutazione finora
- De La Salle University Medical Center Department of Obstetrics and GynecologyDocumento3 pagineDe La Salle University Medical Center Department of Obstetrics and GynecologyNehemiah FranciscoNessuna valutazione finora
- Name: Wong Wai Kheong Matrix No: BMS12081154Documento13 pagineName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNessuna valutazione finora
- Case History For Surg-CVIDocumento12 pagineCase History For Surg-CVIinsulin.baseNessuna valutazione finora
- Case Clerking ApendicDocumento15 pagineCase Clerking ApendicChen Cheng0% (1)
- Duran, Kayllien - Group 7 Sec ADocumento5 pagineDuran, Kayllien - Group 7 Sec AKAYLLIEN DURANNessuna valutazione finora
- Bedside OutputDocumento5 pagineBedside OutputREGENE KRIS SIMMONE GAMILNessuna valutazione finora
- PEDIA Case 4.1. Dengue FeverDocumento10 paginePEDIA Case 4.1. Dengue Feverotartil_nimanNessuna valutazione finora
- Date and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessDocumento3 pagineDate and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessConcepcion R. AquinoNessuna valutazione finora
- IM Gastro FinalDocumento10 pagineIM Gastro FinalIzzyMaxinoNessuna valutazione finora
- I. General DataDocumento6 pagineI. General Datamadison DeliNessuna valutazione finora
- I. General DataDocumento7 pagineI. General Datamadison DeliNessuna valutazione finora
- Soap 2Documento5 pagineSoap 2api-456313554Nessuna valutazione finora
- CaseDocumento2 pagineCaseJim Christian EllaserNessuna valutazione finora
- Final Assessment Soap NoteDocumento13 pagineFinal Assessment Soap Noteapi-494643478100% (3)
- Case Clerking ApendicDocumento15 pagineCase Clerking ApendicMelvin Khung100% (1)
- Mundo - Ob Case 1Documento6 pagineMundo - Ob Case 1Jxyp MundoNessuna valutazione finora
- B6 - Surgery GS II Case IIDocumento10 pagineB6 - Surgery GS II Case IIGregNessuna valutazione finora
- Differential DiagnosisDocumento10 pagineDifferential DiagnosisRhaffy Bearneza RapaconNessuna valutazione finora
- Case Report III Internal MedicineDocumento12 pagineCase Report III Internal MedicineGidu Said0% (1)
- Grand Case PresentationDocumento44 pagineGrand Case PresentationAilyn LoroNessuna valutazione finora
- Team C Final Written OutputDocumento22 pagineTeam C Final Written OutputCarina SuarezNessuna valutazione finora
- Highest Blood Pressure Was 140/90 MMHGDocumento5 pagineHighest Blood Pressure Was 140/90 MMHGFG ArciagaNessuna valutazione finora
- Internal Medicine Cases PresentationsDocumento68 pagineInternal Medicine Cases PresentationsEliudi Kituma100% (2)
- Examples for Sheets (1) باطنةDocumento17 pagineExamples for Sheets (1) باطنةzizoNessuna valutazione finora
- Type The Document Title: Department of Surgery Case Report-IiDocumento10 pagineType The Document Title: Department of Surgery Case Report-IiEyosiyas AbiyNessuna valutazione finora
- Case Report IV Internal MedicineDocumento11 pagineCase Report IV Internal MedicineGidu Said100% (1)
- History and PE Med3ADocumento3 pagineHistory and PE Med3Aawesome avedNessuna valutazione finora
- Case 1 Doc GonsalvesDocumento7 pagineCase 1 Doc GonsalvesMonique Angela Turingan GanganNessuna valutazione finora
- Sample POMRDocumento4 pagineSample POMRJeffrey RamosNessuna valutazione finora
- Case 3Documento10 pagineCase 3atdumagNessuna valutazione finora
- Case Study ClinicalDocumento15 pagineCase Study ClinicalJane FlorendoNessuna valutazione finora
- April 2019 Ent Clerk On Duty: JC Kned JC KnedDocumento1 paginaApril 2019 Ent Clerk On Duty: JC Kned JC Knedk.n.e.d.Nessuna valutazione finora
- Family Medicine - Hospice Care and PalliationDocumento1 paginaFamily Medicine - Hospice Care and Palliationk.n.e.d.Nessuna valutazione finora
- Guidelines For CPCDocumento4 pagineGuidelines For CPCk.n.e.d.Nessuna valutazione finora
- FORENSIC BALLISTIC ReportDocumento3 pagineFORENSIC BALLISTIC Reportk.n.e.d.100% (3)
- IM Patient RRM DOB Cardiomegaly Pulmonary CongestionDocumento3 pagineIM Patient RRM DOB Cardiomegaly Pulmonary Congestionk.n.e.d.Nessuna valutazione finora
- 5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene ManaloDocumento6 pagine5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene Manalok.n.e.d.Nessuna valutazione finora
- Genogram - EsgueraDocumento2 pagineGenogram - Esguerak.n.e.d.Nessuna valutazione finora
- Ob - Postterm Pregnancy - Dr. PastranaDocumento6 pagineOb - Postterm Pregnancy - Dr. Pastranak.n.e.d.Nessuna valutazione finora
- OB HistoryDocumento3 pagineOB Historyk.n.e.d.Nessuna valutazione finora
- Sexual Intercourse: May Result To PREGNANCYDocumento16 pagineSexual Intercourse: May Result To PREGNANCYk.n.e.d.Nessuna valutazione finora
- Timolol Knedrick Kevin C. Macalma FinalDocumento3 pagineTimolol Knedrick Kevin C. Macalma Finalk.n.e.d.Nessuna valutazione finora
- Amoebiasis 6 Buiding BlocksDocumento2 pagineAmoebiasis 6 Buiding Blocksk.n.e.d.Nessuna valutazione finora
- Med Micro Lab Activity #4Documento9 pagineMed Micro Lab Activity #4k.n.e.d.Nessuna valutazione finora
- Lapatinib (KNEDRICK MACALMA)Documento1 paginaLapatinib (KNEDRICK MACALMA)k.n.e.d.Nessuna valutazione finora
- Patient-Centered Family-Focused Community-Oriented: Case: AmoebiasisDocumento3 paginePatient-Centered Family-Focused Community-Oriented: Case: Amoebiasisk.n.e.d.Nessuna valutazione finora
- Family Medicine - Impact of Illness in The Family 01-20-17Documento7 pagineFamily Medicine - Impact of Illness in The Family 01-20-17k.n.e.d.Nessuna valutazione finora
- CASE REPORT On ToxoplasmosisDocumento23 pagineCASE REPORT On Toxoplasmosisk.n.e.d.Nessuna valutazione finora
- Bully Prevention in Positive Bahavior SupportDocumento59 pagineBully Prevention in Positive Bahavior Supportk.n.e.d.Nessuna valutazione finora
- C-Reactive Protein (CRP) Is AnDocumento14 pagineC-Reactive Protein (CRP) Is Anfelipe smithNessuna valutazione finora
- Pedia Drug Study NaproxenparacetamolDocumento3 paginePedia Drug Study NaproxenparacetamolKuro HanabusaNessuna valutazione finora
- Gall Bladder Diseases by - DR Arun Aggarwal GastroenterologistDocumento53 pagineGall Bladder Diseases by - DR Arun Aggarwal GastroenterologistDr. Arun Aggarwal GastroenterologistNessuna valutazione finora
- M S eDocumento87 pagineM S eabhishek agarwalNessuna valutazione finora
- Kehamilan Dengan Hiv: Manggala Pasca WardhanaDocumento38 pagineKehamilan Dengan Hiv: Manggala Pasca WardhanaYudha SatriaNessuna valutazione finora
- EpilepsyDocumento43 pagineEpilepsyMpt SportsNessuna valutazione finora
- Administering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESDocumento14 pagineAdministering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESPb0% (1)
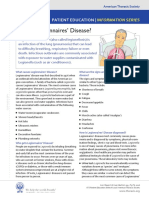
- What Is Legionnaires' Disease?: Patient EducationDocumento2 pagineWhat Is Legionnaires' Disease?: Patient EducationvivaNessuna valutazione finora
- Nursing Responsibilities For Oxygen AdministrationDocumento3 pagineNursing Responsibilities For Oxygen AdministrationJahseh WolfeNessuna valutazione finora
- Pathophysiology Total Anterior Circulation Infarction Left Middle Cerebral Artery (TACILMCA)Documento2 paginePathophysiology Total Anterior Circulation Infarction Left Middle Cerebral Artery (TACILMCA)PATHOSHOPPE100% (1)
- Best Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihDocumento7 pagineBest Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihARS University BandungNessuna valutazione finora
- Wesleyan: College of Nursing and Allied Medical SciencesDocumento2 pagineWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNessuna valutazione finora
- Hinsberg's Method For Characterizing Primary, Secondary, and Tertiary AminesDocumento4 pagineHinsberg's Method For Characterizing Primary, Secondary, and Tertiary AminesTrixy CarreonNessuna valutazione finora
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterDocumento4 pagineNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterJonas BagasNessuna valutazione finora
- 10 Penyakit Terbanyak JKN 2016Documento2 pagine10 Penyakit Terbanyak JKN 2016RSUD dr. H. Soemarno Sosroatmodjo Kuala KapuasNessuna valutazione finora
- Post Partum AssessmentDocumento3 paginePost Partum Assessmentdanica grace gubaNessuna valutazione finora
- MS MR As ArDocumento21 pagineMS MR As ArTamim IshtiaqueNessuna valutazione finora
- Trusted Medical Answers-In Seconds.: General MycologyDocumento19 pagineTrusted Medical Answers-In Seconds.: General MycologyntnquynhproNessuna valutazione finora
- Meningitis QuestionsDocumento2 pagineMeningitis QuestionsAlly JuanezaNessuna valutazione finora
- 9 - Hepatitis B VaccineDocumento1 pagina9 - Hepatitis B VaccineabhivnairNessuna valutazione finora
- Assessment of Subclinical Symptoms PDFDocumento6 pagineAssessment of Subclinical Symptoms PDFPatriciaNessuna valutazione finora
- Epidemiology, Clinical Presentation, and Diagnostic Evaluation of Parapneumonic Effusion and Empyema in Adults - UpToDateDocumento40 pagineEpidemiology, Clinical Presentation, and Diagnostic Evaluation of Parapneumonic Effusion and Empyema in Adults - UpToDateAlejandra LopezNessuna valutazione finora
- Lecture 5 - Whooping CoughDocumento37 pagineLecture 5 - Whooping CoughShaimaa AbdulkadirNessuna valutazione finora
- Endoscopy Consent Form enDocumento1 paginaEndoscopy Consent Form ento van quyenNessuna valutazione finora
- Module 5 HandoutsDocumento2 pagineModule 5 HandoutsJulie Mher AntonioNessuna valutazione finora
- Speech & Language Therapy in Practice, Spring 1999Documento32 pagineSpeech & Language Therapy in Practice, Spring 1999Speech & Language Therapy in PracticeNessuna valutazione finora
- Self-Declaration Form - PHD Students - July 2021Documento2 pagineSelf-Declaration Form - PHD Students - July 2021Pardha SaradhiNessuna valutazione finora
- Syllabus On Inflammatory Bowel DiseaseDocumento9 pagineSyllabus On Inflammatory Bowel DiseasePTDBNessuna valutazione finora
- Hormonal ImbalanceDocumento3 pagineHormonal ImbalanceShan Armaine CabelaNessuna valutazione finora
- UKHSA 12155 Routine Childhood Immunisation Schedule - Feb2022Documento1 paginaUKHSA 12155 Routine Childhood Immunisation Schedule - Feb2022cicitNessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 4.5 su 5 stelle4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (34)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (46)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeDa EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeValutazione: 4.5 su 5 stelle4.5/5 (2)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (44)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDa EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisValutazione: 5 su 5 stelle5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingDa EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingValutazione: 1 su 5 stelle1/5 (2)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Da EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Valutazione: 5 su 5 stelle5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDa EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNessuna valutazione finora
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDa EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsValutazione: 4.5 su 5 stelle4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (254)