Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- MastoiditisDocumento37 pagineMastoiditisAkanksha EkkaNessuna valutazione finora
- Avipattikar ChurnaDocumento3 pagineAvipattikar ChurnadrbhaveshpNessuna valutazione finora
- Premature Cervical DilationDocumento22 paginePremature Cervical DilationJanelle Lois EscolanoNessuna valutazione finora
- Catapres (Clonidine)Documento2 pagineCatapres (Clonidine)Adrianne BazoNessuna valutazione finora
- RanbaxyDocumento5 pagineRanbaxy26449659Nessuna valutazione finora
- Polycythemia.mansfans.comDocumento14 paginePolycythemia.mansfans.comMans FansNessuna valutazione finora
- Swatilekha Das (RN, MSN)Documento20 pagineSwatilekha Das (RN, MSN)sandeepv08Nessuna valutazione finora
- Wall Color of Patients RoomDocumento80 pagineWall Color of Patients RoomHadži Olivera NikolićNessuna valutazione finora
- FiveSibes Live Gib Strong Tell Us About Your K9 Epileptic Survey ResultsDocumento57 pagineFiveSibes Live Gib Strong Tell Us About Your K9 Epileptic Survey ResultsDorothy Wills-RafteryNessuna valutazione finora
- Auto Urine TherapyDocumento130 pagineAuto Urine TherapyBashu Poudel100% (3)
- Classification Des MédicamentsDocumento28 pagineClassification Des MédicamentsGustyl KolinsNessuna valutazione finora
- CPG - Whiplash Associated DisordersDocumento74 pagineCPG - Whiplash Associated DisordersGumDropNessuna valutazione finora
- Early Life Events and Their Consequences For Later Disease A Life History and Evolutionary PerspectiveDocumento19 pagineEarly Life Events and Their Consequences For Later Disease A Life History and Evolutionary PerspectivepomahskyNessuna valutazione finora
- Core Concepts of A Stroke Centered Transactional AnalysisDocumento7 pagineCore Concepts of A Stroke Centered Transactional AnalysisHossein Seify RadNessuna valutazione finora
- 004 General Consent English (Front)Documento2 pagine004 General Consent English (Front)عبدالله الرعويNessuna valutazione finora
- Nikki Sison CVDocumento2 pagineNikki Sison CVyeng botzNessuna valutazione finora
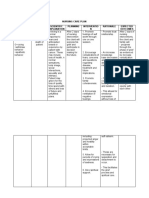
- NCP Case StudyDocumento2 pagineNCP Case StudyGerome Isaiah RabangNessuna valutazione finora
- Role of Food and ExerciseDocumento4 pagineRole of Food and ExerciseShanmugasundaram M Shanmugasundaram MNessuna valutazione finora
- Survey HouseholdDocumento14 pagineSurvey HouseholdACIDNessuna valutazione finora
- Rosenfeld (1984) Hypochondrias, Somatic Delusion and Body Scheme in PsychoanalyticDocumento10 pagineRosenfeld (1984) Hypochondrias, Somatic Delusion and Body Scheme in PsychoanalyticJulián Alberto Muñoz FigueroaNessuna valutazione finora
- Prostate GlandDocumento54 pagineProstate Glanddr_shamimrNessuna valutazione finora
- OPD Claim Form 2020Documento1 paginaOPD Claim Form 2020RafayNessuna valutazione finora
- Clean EatingDocumento92 pagineClean EatingLia Vágvölgyi100% (1)
- Oxytocin and Arginine Vasopressin - A Bridge Between Acupuncture and Autism Spectrum DisorderDocumento6 pagineOxytocin and Arginine Vasopressin - A Bridge Between Acupuncture and Autism Spectrum DisordersovalaxNessuna valutazione finora
- Psychological CausesDocumento3 paginePsychological CausesNINAD NAVANINessuna valutazione finora
- Ancient Mesopotamia Medicine HistoryDocumento4 pagineAncient Mesopotamia Medicine HistoryJhhhcfNessuna valutazione finora
- Enoxaparin FDADocumento40 pagineEnoxaparin FDAImam Nur Alif Khusnudin100% (2)
- NNSC (Northumbria Nutrition Score Chart) : Health and Clinical Excellence) Berdasarkan Reproduktifitas Dan KemudahanDocumento4 pagineNNSC (Northumbria Nutrition Score Chart) : Health and Clinical Excellence) Berdasarkan Reproduktifitas Dan KemudahanYoky AlamsyahNessuna valutazione finora
- Elizabeth L. Samonte BSN Iv Responsibilities of The Nurse To The PatientsDocumento7 pagineElizabeth L. Samonte BSN Iv Responsibilities of The Nurse To The PatientsRein VillanuevaNessuna valutazione finora
- Anti-Aging - UniScience GroupDocumento7 pagineAnti-Aging - UniScience GroupAnonymous 2gIWpUcA8RNessuna valutazione finora