Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Musculoskeletal Fellowship
Caricato da
aristya_tyaCopyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Musculoskeletal Fellowship
Caricato da
aristya_tyaCopyright:
Formati disponibili
Special Ar ticles Original Research
Yablon et al.
Musculoskeletal Fellowship Training
Special Articles
Original Research
A Needs Assessment of
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
Musculoskeletal Fellowship
Training: A Survey of Practicing
Musculoskeletal Radiologists
Corrie M. Yablon1 OBJECTIVE. The purpose of this study was to conduct a needs assessment of musculo-
Jim S. Wu2 skeletal radiologists regarding their musculoskeletal training experience and attitude toward
Lori R. Newman 3 a standardized musculoskeletal fellowship curriculum.
Brian K. Downie1 MATERIALS AND METHODS. An anonymous survey was sent to the Society of
Mary G. Hochman2 Skeletal Radiology membership querying musculoskeletal radiologists practice patterns, fel-
lowship program, curriculum, and modes of learning.
Ronald L. Eisenberg2
RESULTS. Of 216 respondents (26% response rate), 87% were musculoskeletal fellow-
Yablon CM, Wu JS, Newman LR, Downie BK, ship trained. The majority performed MRI, CT, and radiography (99%); arthrography (95%);
Hochman MG, Eisenberg RL spine MRI (77%); pediatric musculoskeletal imaging (75%); musculoskeletal ultrasound
(63%); and biopsies (62%). During fellowship, 72% read spine MRI; 74% pediatric musculo-
skeletal imaging, and 49% musculoskeletal ultrasound (49%); 33% received no spine proce-
dural training. Most felt comfortable performing arthrography, joint injections, and bone and
soft-tissue biopsies but not spine biopsies. Of the total, 33% received a curriculum and 67%
had no formal feedback and 56% did not evaluate their program. The highest rated program
features were teaching by attending physicians (69%), case variety (54%), and procedural
training (49%). The lowest rated features were lack of curriculum (57%), lack of structured
learning (48%), and lack of mentoring (24%). The favorite mode of learning was one-on-one
readout with attending physicians (90%), and 85% agreed that a standardized musculoskele-
tal fellowship curriculum would benefit musculoskeletal training.
CONCLUSION. Although musculoskeletal radiologists believe they were adequately
trained for practice, there are perceived deficiencies in spine MRI, pediatric musculoskeletal
imaging, and musculoskeletal ultrasound. A standardized musculoskeletal fellowship curric-
ulum would provide improved structure and a defined educational program. Clear expecta-
Keywords: fellowship education, musculoskeletal
tions, performance assessment, feedback, and programmatic evaluation should be core ele-
fellowship curriculum, musculoskeletal fellowship ments of the training of every musculoskeletal fellow.
education
M
usculoskeletal fellowship training [2]. Although the SSR has created a curriculum
DOI:10.2214/AJR.12.9105
has been characterized by a di- structured around the ACGME core competen-
Received April 20, 2012; accepted after revision versity of educational experienc- cies for musculoskeletal radiology residency
June13,2012. es. Data obtained in 2012 from the learning [1], there are no formal curricula at
1
Society of Skeletal Radiology (SSR), the major the fellowship level. Even the guidelines for
Department of Radiology, University of Michigan, 1500 E
subspecialty society of musculoskeletal radi- ACGME-accredited fellowships only refer to lo-
Medical Center Dr, Ann Arbor, MI. Address correspond-
ence to C. M. Yablon (cyablon@umich.edu). ology in the United States, listed 14 Accredita- gistics and not to a specific curriculum, which
tion Council of Graduate Medical Education is left to the individual programs to determine
2
Department of Radiology, Beth Israel Deaconess (ACGME)-accredited programs and 64 non- [3]. Non-ACGMEaccredited fellowships are
Medical Center, Harvard Medical School, Boston, MA. ACGME programs, offering a total of 184 posi- not required to follow these guidelines; there-
3
Shapiro Institute for Medical Education and Research at
tions [1]. Since 2010, there has been an increase fore, there are no didactic requirements, and
Harvard Medical School and Beth Israel Deaconess in non-ACGME positions from 123 to 163 [1, 2]. learning experiences are highly unstructured.
Medical Center, Boston, MA. The challenge facing all non-ACGMEac- Most educational material is case based and de-
credited fellowships, not only musculoskeletal termined by the expertise of local attending phy-
AJR 2013; 200:732740
fellowships, is that there is no governing body to sicians, referral patterns, and case volume, with
0361803X/13/2004732 provide uniform guidelines for call duties, work- some fellowships similar to apprenticeships.
ing conditions, compensation, educational pro- In light of the variability of musculoskele-
American Roentgen Ray Society grams, and curricula, which now vary widely tal fellowship educational programming and
732 AJR:200, April 2013
Musculoskeletal Fellowship Training
80 Academic
40 05 years
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
Private practice
610 years
70
35
1115 years
60
30 1620 years
Respondents (%)
Respondents (%)
50
25
40
20
15 30
10 20
5 10
0 0
05 610 1115 1620 020 2140 4160 6180 81100
Time (y) Time (y)
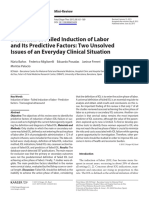
Fig. 1Chart shows percentage of respondents grouped by number of years past Fig. 2Graph shows musculoskeletal radiologists in private practice versus
training. academic practice grouped by percentage of practice time spent subspecializing
in musculoskeletal related activities.
the predominance of non-ACGMEaccredited determine p values. Analyses were performed us- in private practice, 26% worked in small (1- to
fellowships, we sought to assess the perceived ing SAS, version 9.2, statistical software. 10-person) practices, 30% worked in medium
preparedness of musculoskeletal radiologists sized (11- to 20-person) practices, and 44%
and whether a standardized musculoskeletal Results worked in larger sized (> 21-person) practic-
curriculum would be beneficial. We hypothe- Respondent Characteristics es. The respondents had a wide range of years
sized that although musculoskeletal fellowships We sent the survey electronically to 844 of practice experience (Fig. 1).
may provide sufficient preparation for practice, SSR members and received 216 responses, Most of the respondents considered them-
there are knowledge, skill, and attitudinal de- yielding a response rate of 26%. Of those re- selves musculoskeletal subspecialists (87%),
ficiencies that should be identified, addressed, sponding, 87% were musculoskeletal fellow- and many (46%) spent 81100% of their total
and incorporated into a standardized musculo- ship trained, 46% were in an academic prac- practice in musculoskeletal imaging. Most mus-
skeletal fellowship curriculum. tice, and 54% were in private practice. Of the culoskeletal radiologists in academics spent the
97 respondents in academics, 13% had not re- majority of their practice time subspecializing in
Materials and Methods ceived musculoskeletal fellowship training, musculoskeletal imaging; whereas those radiol-
The institutional review board of our hospi- primarily due to the absence of formal muscu- ogists in private practice spent varying degrees
tal deemed our study exempt from further review. loskeletal fellowships before 1986 when mus- of time in musculoskeletal imaging (Fig. 2).
We developed a 36-question survey that included culoskeletal training consisted of apprentice- Ninety-nine percent of respondents per-
multiple choice, yes-or-no, and 5-point Likert scale ship or mentorship models. Of the respondents formed extremity MRI, CT, and radiography
questions. Targeted to practicing musculoskeletal
radiologists, the survey queried radiologists cur-
80
rent practice patterns, fellowship training program Private practice
and curriculum, views on preparedness after train- Academic
Fellowship
ing, and preferred modes of learning. The word
60
curriculum was defined as a directed course of
Respondents (%)
study or core educational content with stated learn- Fig. 3Chart shows
comparison of percentage
ing goals and objectives for a learner to master. of respondents who read 40
The survey was piloted before general testing and spine MRI, pediatric
then distributed electronically through the SSR to musculoskeletal imaging,
and musculoskeletal
its entire membership in April 2011 (Appendix 1). ultrasound in private 20
An accompanying cover letter notified potential re- practice versus academics,
spondents that the results were being collected for compared with the
percentage of respondents
research purposes and would be shared with the 0
who learned those
SSR and academic community. We used chi-square modalities in fellowship Spine Pediatric Musculoskeletal
training. MRI Musculoskeletal Ultrasound
tests and Fisher exact tests for statistical analysis to
AJR:200, April 2013 733
Yablon et al.
in their practices; 95% arthrography; 77% Only 74% of respondents received training in station. Fellows were also required to teach
spine MRI; 75% pediatric musculoskeletal pediatric musculoskeletal imaging; 72% of medical students at the workstation (44%)
imaging; 63% musculoskeletal ultrasound; respondents received training in spine MRI; and to give medical student lectures (37%).
62% imaging-guided biopsy of the extremi- and 49% received training in musculoskeletal When queried about the most outstand-
ties and pelvis; and 40% imaging-guided bi- ultrasound (Fig. 3). ing aspects of the fellowship, the top three
opsies of the spine. responses were teaching by attending phy-
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
Roughly half of the respondents did not per- Evaluation of Fellows and the Fellowship Program sicians (69%), variety of cases (54%), and
form spine procedures. In these cases, these Procedural logs were maintained by only training in procedures (49%). When asked
procedures were performed by several oth- 36% of fellows. The majority of fellows (53%) about the three least-liked aspects of the fel-
er providers, including neuroradiology (71%), received informal feedback during their fel- lowship, respondents most often noted lack
pain medicine (51%), anesthesia (39%), neuro- lowship; 33% of fellows received feedback of a curriculum (57%), lack of a structured
surgery (32%), and physiatry or physical medi- from fellowship directors at regular intervals, learning environment (48%), and lack of
cine and rehabilitation (15%). Nine percent of 27% of fellows received occasional informal help finding a job after fellowship (24%).
respondents replied that spine procedures were feedback, and 12% received no feedback (re- Respondents were asked to rank favored
not performed in their hospital. spondents could provide more than one an- modes of learning. One-on-one readout with
swer). Only 44% of respondents were provid- attending physicians was by far the most pre-
Fellowship Training ed the opportunity to evaluate their program. ferred mode of learning (90%); less popu-
The majority of the musculoskeletal fel- Faculty mentors were assigned to 40% of re- lar modes were reading textbooks at home
lowships were small: 30% had only one fel- spondents. Procedural skills were evaluated (42%), interdisciplinary conferences (39%),
low, 32% had two fellows, 25% had 3 or 4 fel- by faculty in 78% of respondents. Interpreta- just-in-time learning (looking up items on-
lows, and 13% had five or more. The majority tive skills were quantitatively evaluated (i.e., line or in books as questions arose during
of fellowships (54%) had four or fewer attend- competency test, other grading scheme) in 7% readout) (38%), journal and review articles
ing physicians. Twenty-eight percent had 5 or of respondents. (37%), and didactic conferences (34%). Sur-
6 attending physicians, 13% had 79, and 5% prisingly, online teaching modules were the
had 10 or more attending physicians. Curriculum least-favored activity (only 3%).
Spine procedural training was variable A curriculum, or learning goals and objec- Respondents wished they had received
across fellowships. Thirty-two percent of re- tives for the core educational content of the more training during fellowship in the follow-
spondents received no spine procedure training fellowship program, were presented to 33% ing modalities: musculoskeletal ultrasound
at all. Of those receiving spine procedure train- of those responding. Of the remaining 67% of (56%), pediatrics (43%), bone biopsies (32%),
ing, 51% learned spine biopsies, 43% learned respondents, 14% were given a list of muscu- spine MRI (26%), dual-energy x-ray absorp-
epidural steroid injections, 54% learned to do loskeletal topics they were expected to know tiometry (23%), musculoskeletal MRI (21%),
facet injections, 22% performed vertebroplas- by completion of the fellowship. A structured and soft-tissue biopsies (21%). Respondents
ty, and 12% performed kyphoplasty. conference schedule was provided to 67% of were queried about their feelings of prepared-
When asked if they received adequate respondents. Conferences included orthope- ness to practice radiology after fellowship,
training to feel comfortable performing pro- dic oncology or tumor board (77%), rheuma- attitudes toward fellowship training, and a
cedures in practice, the majority of respon- tology (67%), sports medicine (50%), journal standardized musculoskeletal fellowship cur-
dents replied that they felt adequately or even club (45%), didactics (43%), quality assurance riculum (Table 1). Overall, the majority of
better trained than colleagues in their prac- (34%), and follow-up conferences (28%). respondents felt well-prepared for practice,
tices to perform arthrography (99%); joint in- thought musculoskeletal fellowship training
jections (97%); and biopsies of bone (78%), Learning and Attitudes was optimal for the practice of musculoskel-
soft tissue (81%), and spine (49%). Regarding When taught how to perform procedures, etal radiology, and favored the creation of a
cross-sectional studies (CT and MRI exami- 31% practiced biopsies on a phantom be- standardized musculoskeletal fellowship cur-
nations), 91% of respondents thought they had fore performing biopsies. Most respondents riculum. There was no statistical correlation
read sufficient examinations to feel adequate- (88%) were required to teach during fellow- between respondents receiving a curriculum
ly prepared for practice; 89% thought they ship, with 73% required to give resident lec- and perceived preparedness for practice (p<
had read a sufficient number of radiographs. tures and 71% to teach residents at the work- 1.0)the reason being that all musculoskel-
TABLE 1: Respondents Views of Musculoskeletal Fellowship Training and Musculoskeletal Fellowship Curriculum
Survey Statement Response
Compared with other colleagues in your current practice, how Much more prepared (42) More prepared (29) Equally prepared (27) Less prepared (3)
well prepared for practice of musculoskeletal radiology did you
feel after completing your fellowship?
Musculoskeletal fellowship training is the optimal training for Strongly agree (65) Agree (32) Disagree (1) Strongly disagree (2)
pursuing musculoskeletal radiology in practice.
A standardized musculoskeletal fellowship curriculum would be Strongly agree (27) Agree (58) Disagree (11) Strongly disagree (4)
beneficial to musculoskeletal fellowship training.
NoteData in parentheses are percentages.
734 AJR:200, April 2013
Musculoskeletal Fellowship Training
etal-trained respondents except four felt pre- ple read pediatric musculoskeletal imaging respectively, as the favored learning method.
pared for practiceor their perceived need studies, and a similar number received fellow- Web-based learning also did not score highly,
for a standardized curriculum (p< 0.4305). ship training in this area; however, although which is surprising given the digital nature of
There also was no relationship between years 63% perform musculoskeletal ultrasound in radiology. This finding may be explained by the
after training and the desire for a standardized their practices, only 49% received training in heterogeneous quality of web-based offerings
curriculum (p= 0.3809). this area during fellowship. This suggests that for musculoskeletal imaging; the (often time-
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
The top five factors influencing the deci- musculoskeletal fellowship training programs consuming) need to search multiple sources to
sion to choose a job were the following: loca- should offer elective rotations in pediatric find credible, referenced material; and the lack
tion (75%), colleagues at the future location musculoskeletal imaging and musculoskeletal of material directed at the fellowship level.
(42%), income (25%), desire for an academic ultrasound if these areas are not already a part In retrospect, respondents wished they had
practice (24%), and work hours (23%). Nei- of the standard curriculum. received more training in musculoskeletal ul-
ther faculty mentors nor fellowship-related Our study revealed room for improvement trasound, pediatric musculoskeletal imaging,
clinical, educational, or research experiences regarding formal procedural and interpretive bone biopsies, spine MRI, dual-energy x-ray
figured prominently in the decision to choose skills assessment and feedback to fellows, absorptiometry, musculoskeletal MRI, and
a postition. which can provide valuable teaching and in- soft-tissue biopsies. These findings likely re-
sight [7, 8]. Although the ACGME requires flect the changing landscape of musculoskeletal
Discussion quarterly feedback of residents and fellows radiology. Both academic and private practic-
Past studies of musculoskeletal fellowship [3], only 33% of respondents received formal es are performing more musculoskeletal ultra-
programs have focused on surveying the pro- feedback at regular intervals, with the remain- sound. Pediatric musculoskeletal imaging is
gram directors or fellows in training. A 1998 der receiving only informal feedback. Feed- ubiquitous in private practice and community
survey of fellowship program directors as- back should be scheduled quarterly, discussed hospitals. Musculoskeletal interventions are in-
sessed the status of the programs training and in a private setting, and documented in writ- creasing, and requests for percutaneous biop-
supervision with a focus on ACGME accredi- ing. Fellows should also be given the opportu- sies of bone and soft-tissue masses of the ex-
tation [4]. A subsequent 2003 study surveyed nity to evaluate the program, which is another tremities are commonplace in many practices.
program directors to compare the structure ACGME requirement [3]. In our experience, Musculoskeletal specialists are well positioned
of ACGME to non-ACGMEaccredited pro- these types of evaluation sessions have led to to partner with orthopedic surgeons to plan in-
grams [5]. An unpublished 2010 abstract sur- positive change and training improvement. terventions and perform posttreatment imaging.
veyed fellows in the first few months of train- There has been debate in the musculo- Many orthopedic surgeons order spine MRI as
ing regarding factors influencing their choice skeletal community regarding the utility of part of their practice, and musculoskeletal ra-
of fellowship, their attitudes toward a fellow- having a standardized musculoskeletal im- diologists can increase their consultative value
ship match, program logistics, and receptivity aging fellowship curriculum. No formal cur- to their orthopedic colleagues by interpreting
toward a fellowship curriculum (Rao N et al., riculum currently exists, and our survey in- these as well as extremity studies.
presented at the 2010 annual meeting of the dicates that most programs devise their own Most musculoskeletal radiologists surveyed
SSR). This is the first study to assess the opin- curricula, if any. This leads to a heterogene- thought that musculoskeletal fellowships pre-
ions of practicing radiologists regarding their ous learning experience that is dependent on pared them well for practice, despite the dif-
fellowship training and whether it adequately the specific fellowship chosen. If there were ferences among fellowships. However, the
prepared them for practice. By surveying radi- a standard curriculum, self-directed learners majority thought that a standardized musculo-
ologists in practice, we had the opportunity to could identify and fill programmatic gaps skeletal fellowship curriculum would provide
query those who had gained perspective over or seek radiology experience not offered on further benefit. Although fellows likely sup-
time as to the best educational methods to use site. It is noteworthy that when queried about plement their own learning when modalities
and whether a standard curriculum would ben- the three things they liked least about their or subjects are not covered in their programs,
efit fellowship training. fellowships, the two major complaints were the presence of a structured curriculum would
This survey revealed important findings lack of a curriculum (57%) and lack of a enhance the learning experience and provide
to help structure future fellowship programs. structured learning environment (48%). a guide for specific topics that should be cov-
For example, 77% of respondents continue It is not surprising that the respondents fa- ered during fellowship.
to read spine MRI both in academic and in vored mode of learning was one-on-one read- When the initial results of this survey were
private practices, and 40% perform imaging- out with an attending physician. Despite ad- shared with members of the SSR community
guided biopsies of the spine. This indicates vances in digital teaching methods, one-on-one in late 2011 and early 2012, the SSR Education
that spine interpretation and procedures re- teaching during readouts remains the primary Committee and others in the musculoskeletal
main a significant and valuable aspect of method of teaching radiology and imparting the academic community agreed that the prelimi-
musculoskeletal imaging, and thus training subtleties of radiologic interpretation. One-on- nary findings confirmed the need to draft fel-
in this area should be an essential part of a one interaction with a supportive instructor or lowship curricular guidelines or suggestions.
musculoskeletal fellowship. mentor is an immediate and gratifying way to
Pediatric musculoskeletal studies are com- learn, in which years of the instructors expe- Limitations
monly interpreted in private practice and mus- rience can be distilled into focused teaching at Given the moderate (26%) response rate,
culoskeletal ultrasound use has grown both in the workstation. Reading textbooks at home, we likely encountered some selection bias. The
academic and private practices during the past just-in-time learning, and reading journal arti- SSR is a self-selected group of musculoskele-
decade [6]. Seventy-five percent of our sam- cles ranked a distant second, third, and fourth, tal subspecialists who have a stated interest in
AJR:200, April 2013 735
Yablon et al.
musculoskeletal imaging and therefore affiliate well for practice. However, there are perceived skeletal radiology. www.acgme.org/acgmeweb/
with the organization. There are likely many educational deficiencies in spine MRI, pedi- Portals/0/PFAssets/ProgramRequirements/426_
more self-identified musculoskeletal-trained ra- atric musculoskeletal imaging, and musculo- musculoskeletal_diag_rad_07012010_1-YR.pdf.
diologists, unaffiliated with the SSR, who were skeletal ultrasound as well as, less frequently, Published July 1, 2010. Accessed December 4,
unable to participate in this study because their bone, soft-tissue, and spine biopsies. These de- 2012
identity and contact information were not read- ficiencies may be corrected by the creation of 4. De Smet AA, Resnik CS. Current status of mus-
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
ily available. For ease of distribution, we chose a standardized musculoskeletal fellowship cur- culoskeletal radiology fellowships in the United
to send the survey through the SSR to provide a riculum that provides improved structure and a States. Acad Radiol 1998; 5:509512
roughly equal mix of private practice and aca- defined educational program. Didactics aimed 5. Berquist TH, Bancroft LW, Kransdorf MJ, Ander-
demic musculoskeletal radiologists. Moreover, at the fellowship level should be incorporat- son MR, Walters RM. Postgraduate musculoskel-
we thought that musculoskeletal radiologists ed into the program. Clear expectations, per- etal fellowship training in the United States: cur-
affiliated with the SSR most likely had a vested formance assessment, feedback, and program- rent trends and future direction. Skeletal Radiol
interest in the future of musculoskeletal educa- matic evaluation should be core elements of the 2003; 32:337342
tion and were more likely to respond. training of every musculoskeletal fellow. 6. Sharpe RE, Nazarian LN, Parker L, Rao VM,
Surveys on fellowship education may cre- Levin DC. Dramatically increased musculoskele-
ate recall bias in that the respondents tend to References tal ultrasound utilization from 2000 to 2009, es-
recall their training favorably as a reflection 1. Society of Skeletal Radiology website. MSK fel- pecially by podiatrists in private offices. J Am
of good decision making on their part. In ad- lowships. skeletalrad.org/resources/fellowships. Coll Radiol 2012; 9:141146
dition, respondents may not accurately recall aspx. Published March 19, 2012. Accessed April 7. Ende J. Feedback in clinical medical education.
the details of their fellowship training as the 4, 2012 JAMA 1983; 250:777781
time of training grows more remote. 2. Baker SR, Luk L, Clarkin K. The trouble with fel- 8. Yarris LM, Fu R, LaMantia J, et al. Effect of an
lowships. J Am Coll Radiol 2010; 7:446451 educational intervention on faculty and resident
Conclusion 3. Accreditation Council of Graduate Medical Educa- satisfaction with real-time feedback in the emer-
Practicing radiologists believe that musculo- tion (ACGME) website. ACGME program require- gency department. Acad Emerg Med 2011;
skeletal fellowship training has prepared them ments for graduate medical education in musculo- 18:504512
Appendix 1: Musculoskeletal Curriculum Survey
Part I: Tell us about yourself and your practice
1. Did you do a musculoskeletal imaging fellowship?
a. Yes
b. No
2. If you did not do a musculoskeletal fellowship, please describe any training after residency:
3. How many years ago did you complete your training after fellowship?
a. 02 years
b. 35 years
c. 610 years
d. 1115 years
e. 16 or more years ago
4. Please select your current practice type:
a. Small private practice (010)
b. Medium private practice (1120)
c. Large private practice (> 21)
d. Academics
e. I am not practicing radiology
f. Other (please specify)
5. What percentage of your total practice do you devote to musculoskeletal studies (includes extremity and spine, both diagnostic and therapeutic)?
a. 020%
b. 2140%
c. 4160%
d. 6180%
e. 81100%
(Appendix continues on next page)
736 AJR:200, April 2013
Musculoskeletal Fellowship Training
Appendix 1: Musculoskeletal Curriculum Survey (continued)
6. Please indicate which of the following modalities you currently perform in your practice (please check all that apply):
a. Pediatric musculoskeletal
b. Musculoskeletal CT
c. Imaging-guided biopsies of the extremities and pelvis
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
d. Extremity MRI
e. Spine MRI
f. Arthrography
g. Musculoskeletal radiography
h. Musculoskeletal ultrasound
i. Imaging-guided biopsies of the spine
7. If you do not perform spine procedures in your practice, who does perform them?
a. Neuroradiology
b. Neurosurgery
c. Anesthesia
d. Physiatry/Physical Medicine and Rehabilitation service
e. Pain Medicine
f. We do not perform these in our hospital
Part II. Your fellowship training program
1. If you did a musculoskeletal fellowship, how big was your program?
a. One fellow
b. Two fellows
c. Three or four fellows
d. Five or more fellows
2. How many musculoskeletal attending physicians were on staff in your program?
a. Four or fewer
b. Five or six
c. Seven to nine
d. 10 or more
3. Did you read or perform the following in your fellowship (please check all that apply)?
a. Spine MRI
b. Pediatric musculoskeletal studies
c. Musculoskeletal ultrasound
4. Were you offered the opportunity to do the following (check all that apply)?
a. Epidural injections
b. Facet injections
c. Spine biopsies
d. Vertebroplasty
e. Kyphoplasty
f. Other (please specify)
g. None of the above
5. Did you get adequate training to feel comfortable to perform the following procedures in practice:
Inadequate Adequate More than adequate
Arthrography
Joint injections
Bone biopsies
Soft-tissue biopsies
Spine biopsies
6. Were you required to keep a procedure log during your fellowship?
a. Yes
b. No
(Appendix continues on next page)
AJR:200, April 2013 737
Yablon et al.
Appendix 1: Musculoskeletal Curriculum Survey (continued)
7. Please rank the top three things you found most outstanding about your musculoskeletal fellowship training (three is most outstanding)?
Mentorship in finding a job after fellowship
Curriculum
Wide variety of cases
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
Supportive learning environment
Preparation for practice beyond fellowship
Training in procedures
Teaching by attending physicians
Appropriate volume of cases
Structured learning environment
Other (please specify)
8. Please rank the three things you found least desirable about your musculoskeletal fellowship training (one is least desirable).
Lack of help finding a job after fellowship
Lack of a curriculum
Lack of variety of cases
Lack of preparation for practice beyond fellowship
Lack of training in procedures
Not enough individualized attention
Not enough teaching
Too high volume of cases
Too low volume of cases
Lack of structured learning environment
Other (please specify)
9. Did you receive feedback on your performance during your fellowship (you may check more than one)?
a. Yes, by the fellowship director(s) at regular intervals
b. Yes, by the attending physicians in an informal manner
c. Yes, I received occasional feedback
d. No, I did not receive feedback
10. Were you given the opportunity to provide an evaluation of your program to your program director(s)?
a. Yes
b. No
11. A re there any other aspects of fellowship training that you would have liked to have received before entering practice? Please specify.
Part III: Curriculum/learning
A curriculum is defined as a directed course of study or core educational content with stated learning goals and objectives for a learner
to master.
1. At the beginning of your fellowship, were you presented with learning goals and objectives for the programs core educational content?
a. Yes
b. No
2. If you answered no to the previous question, were you given a list of topics in musculoskeletal radiology that you were expected to
know by the end of your fellowship?
a. Yes
b. No
3. Did you have an assigned faculty mentor with whom you worked on a regular basis?
a. Yes
b. No
4. Were you taught how to perform procedures (e.g., practice a biopsy on a phantom) before working on a patient?
a. Yes
b. No
5. Were your procedural skills evaluated by faculty?
a. Yes
b. No
(Appendix continues on next page)
738 AJR:200, April 2013
Musculoskeletal Fellowship Training
Appendix 1: Musculoskeletal Curriculum Survey (continued)
6. Were your interpretive skills evaluated quantitatively? (e.g., a competency test, MRI examinations to interpret for grading, etc.)
a. Yes
b. No
7. Please rank, in order of importance, your top three preferred modes of learning during your fellowship.
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
a. Didactic conferences
b. Just-in-time learning, (e.g., looked up topics on Internet, in books, online teaching modules) as questions arose during readout
c. Online search/Google/Wikipedia, etc.
d. Read textbooks at home
e. Online teaching modules
f. One-on-one readout/teaching at the monitor with attending physician
g. Journal articles/review articles
h. Interdisciplinary conferences
i. Curriculum provided by the program
Part IV: Conferences
1. Did your fellowship have a structured conference schedule?
a. Yes
b. No
2. Did your program provide the following (check all that apply)?
a. Quality assurance
b. Orthopedic oncology/tumor board
c. Rheumatology conference
d. Sports medicine conference
e. Spine conference
f. Didactic conferences for fellows
g. Journal club
h. Follow-up conferences
i. None of the above
j. Other (please specify)
3. Were you required to teach others during your fellowship (check all that apply)?
a. Medical student lectures
b. Radiology resident lectures
c. Other resident lectures
d. Departmental CME course
e. Taught medical students at the PACS workstation
f. Taught residents at the PACS workstation
g. I was not required to teach
Part V: Reflections on your fellowship
1. Did you feel you read an adequate number of radiographs in fellowship to be prepared for practice after fellowship?
Strongly agree Agree Disagree Strongly disagree
2. In your opinion, did you read a sufficient number of musculoskeletal cross-sectional studies in your fellowship to prepare you for practice
after training?
Strongly agree Agree Disagree Strongly disagree
3. Please rate how comfortable you felt performing the following procedures on completing fellowship:
Very uncomfortable Uncomfortable Comfortable Very comfortable
Arthrography
Imaging-guided biopsy of the extremities
Imaging-guided biopsy of the spine
(Appendix continues on next page)
AJR:200, April 2013 739
Yablon et al.
Appendix 1: Musculoskeletal Curriculum Survey (continued)
4. In which areas do you wish you had received more training? Check all that apply:
a. I felt perfectly trained in everything
b. Musculoskeletal MRI
c. Musculoskeletal CT
Downloaded from www.ajronline.org by 180.245.204.167 on 11/28/17 from IP address 180.245.204.167. Copyright ARRS. For personal use only; all rights reserved
d. Radiography
e. Arthrography
f. Bone biopsies
g. Soft-tissue biopsies
h. Spine MRI
i. Spine biopsies
j. Musculoskeletal ultrasound
k. Dual-energy x-ray absorptiometry
l. Pediatric musculoskeletal
5. Compared with other colleagues in your current practice, how well prepared for practice of musculoskeletal radiology did you feel after
completing your fellowship?
Much less prepared Less prepared Equally prepared More prepared Much more prepared
6. Please indicate your agreement or disagreement with the following statement: Completing a musculoskeletal fellowship is optimal train-
ing for the practice of musculoskeletal radiology.
Strongly agree Agree Disagree Strongly disagree
7. Please state your agreement or disagreement with the following statement: A standardized musculoskeletal fellowship curriculum would
be beneficial to fellowship training.
Strongly agree Agree Disagree Strongly disagree
Part VI: Life after training
1. Please rank, in order of importance, the top three factors that influenced your choice of job after fellowship:
a. Faculty mentor
b. Clinical experience during fellowship
c. Educational experience during fellowship
d. Research experience during fellowship
e. Income
f. Work hours
g. Spouses career/employment
h. Medical school debt
i. Location
j. Really wanted an academic job
k. Really wanted a private practice job
l. People at future job
m. Other (please specify)
740 AJR:200, April 2013
Potrebbero piacerti anche
- Definition of Failed Induction of Labor and Its Predictive Factors: Two Unsolved Issues of An Everyday Clinical SituationDocumento10 pagineDefinition of Failed Induction of Labor and Its Predictive Factors: Two Unsolved Issues of An Everyday Clinical Situationaristya_tyaNessuna valutazione finora
- Circulatory ShockDocumento9 pagineCirculatory ShockTri UtomoNessuna valutazione finora
- Pain On Injection of Propofol: Efficacy of Paracetamol and LidocaineDocumento7 paginePain On Injection of Propofol: Efficacy of Paracetamol and LidocaineBadrun IbrahimNessuna valutazione finora
- Colonic Intussusception: Clinical and Radiographic Features: Marc J. GollubDocumento6 pagineColonic Intussusception: Clinical and Radiographic Features: Marc J. GollubvinaNessuna valutazione finora
- On Call MusculoskeletalDocumento4 pagineOn Call Musculoskeletalaristya_tyaNessuna valutazione finora
- Roloff Et Al-2015-International Journal of Gynecology & ObstetricsDocumento5 pagineRoloff Et Al-2015-International Journal of Gynecology & Obstetricsaristya_tyaNessuna valutazione finora
- Focused Impact On MRI PDFDocumento9 pagineFocused Impact On MRI PDFaristya_tyaNessuna valutazione finora
- Initial Radiographic Features As Outcome Predictor of Adult Respiratory Syncytial Virus Respiratory Tract InfectionDocumento7 pagineInitial Radiographic Features As Outcome Predictor of Adult Respiratory Syncytial Virus Respiratory Tract Infectionaristya_tyaNessuna valutazione finora
- Jurnal Pendidikan KimiaDocumento9 pagineJurnal Pendidikan KimiaWike Irdyy TambayongNessuna valutazione finora
- Initial Radiographic Features As Outcome Predictor of Adult Respiratory Syncytial Virus Respiratory Tract InfectionDocumento7 pagineInitial Radiographic Features As Outcome Predictor of Adult Respiratory Syncytial Virus Respiratory Tract Infectionaristya_tyaNessuna valutazione finora
- Iwan RioDocumento10 pagineIwan Rioaristya_tyaNessuna valutazione finora
- JefA TerjemahanDocumento10 pagineJefA Terjemahanaristya_tyaNessuna valutazione finora
- Influence of Applying NitroglycerinDocumento6 pagineInfluence of Applying Nitroglycerinaristya_tyaNessuna valutazione finora
- Serviksitis originality reportDocumento5 pagineServiksitis originality reportaristya_tyaNessuna valutazione finora
- DNA Microarrays: Patrick Schmid CSE 497 Spring 2004Documento14 pagineDNA Microarrays: Patrick Schmid CSE 497 Spring 2004aristya_tyaNessuna valutazione finora
- DNA Sequencing MethodsDocumento6 pagineDNA Sequencing Methodsaristya_tyaNessuna valutazione finora
- Aneurysma AortDocumento22 pagineAneurysma Aortaristya_tyaNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar Pustakaaristya_tyaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- RAMOS VS CA, 380 SCRA 467: FactsDocumento2 pagineRAMOS VS CA, 380 SCRA 467: FactsEarvin Joseph BaraceNessuna valutazione finora
- POCUSDocumento10 paginePOCUSSMIBA MedicinaNessuna valutazione finora
- DR UsmanDocumento7 pagineDR Usmanusman_rana84Nessuna valutazione finora
- Saint Paul University Philippines: Tuguegarao City, Cagayan 3500Documento1 paginaSaint Paul University Philippines: Tuguegarao City, Cagayan 3500Divine Cagayan SuyuNessuna valutazione finora
- List of Registered ParticipantsDocumento32 pagineList of Registered Participantsraj RajputNessuna valutazione finora
- The International Journal of Periodontics & Restorative DentistryDocumento10 pagineThe International Journal of Periodontics & Restorative Dentistrykevin1678Nessuna valutazione finora
- Policies and Procedures On Continuous Quality ImprovementDocumento16 paginePolicies and Procedures On Continuous Quality ImprovementSooraj ThomasNessuna valutazione finora
- SAIL Guide Book PDFDocumento58 pagineSAIL Guide Book PDFRam Suresh Tiwari33% (3)
- Nursing Care Plan for Imbalanced NutritionDocumento2 pagineNursing Care Plan for Imbalanced NutritionCuttie Anne GalangNessuna valutazione finora
- Health BandDocumento4 pagineHealth BandMichael Jay KennedyNessuna valutazione finora
- Landmark Cases in Forensic PsychiatryDocumento241 pagineLandmark Cases in Forensic PsychiatryKyiubi el mundoNessuna valutazione finora
- File Thuyết TrìnhDocumento3 pagineFile Thuyết TrìnhBích TuyềnNessuna valutazione finora
- Psychiatric History 1Documento6 paginePsychiatric History 1Stephen Jao Ayala UjanoNessuna valutazione finora
- List of Current Aeromedical Examiners as of 2010Documento26 pagineList of Current Aeromedical Examiners as of 2010naveenbalaNessuna valutazione finora
- Ethiopian Journal PediatricDocumento78 pagineEthiopian Journal PediatricZulia Ahmad BurhaniNessuna valutazione finora
- النسخه الثالثه نواف الحارثي ٢٠١٩Documento92 pagineالنسخه الثالثه نواف الحارثي ٢٠١٩Atheer AlsalehNessuna valutazione finora
- Drug Study IbuprofenDocumento3 pagineDrug Study IbuprofenblaireNessuna valutazione finora
- Sterne 2020Documento3 pagineSterne 2020GARINDA ALMA DUTANessuna valutazione finora
- Inauguration Presentation - Growth & ExcellenceDocumento13 pagineInauguration Presentation - Growth & Excellenceqazi1975Nessuna valutazione finora
- Convocation Medal ListDocumento18 pagineConvocation Medal ListVidya SagarNessuna valutazione finora
- Attracting and Retaining Healthcare StaffDocumento9 pagineAttracting and Retaining Healthcare StaffAnonymous MFh19TBNessuna valutazione finora
- Introduction To Regulatory AffairsDocumento15 pagineIntroduction To Regulatory AffairsCyclone Pharmaceuticals Pvt Ltd PuneNessuna valutazione finora
- The Impact of Fitness On Surgical Outcomes The.14Documento8 pagineThe Impact of Fitness On Surgical Outcomes The.14MIGUEL MORENONessuna valutazione finora
- Clinical Biochemistry HSST CurriculumDocumento111 pagineClinical Biochemistry HSST CurriculumChengyuan ZhangNessuna valutazione finora
- Reverse Pharmacology: Integrating Traditional Medicine into Modern Drug DevelopmentDocumento27 pagineReverse Pharmacology: Integrating Traditional Medicine into Modern Drug DevelopmentGourisankar RoulNessuna valutazione finora
- Stem Cell TherapyDocumento3 pagineStem Cell TherapyDr DumitrescuNessuna valutazione finora
- Pharmacist Code of EthicsDocumento12 paginePharmacist Code of EthicsShimul HalderNessuna valutazione finora
- Advocacy Activities On Tobacco Prevention and ControlDocumento27 pagineAdvocacy Activities On Tobacco Prevention and ControlKristine AguilarNessuna valutazione finora
- Orientation to Pharmacy DepartmentDocumento17 pagineOrientation to Pharmacy DepartmentAliNessuna valutazione finora
- Physician's Order SummaryDocumento4 paginePhysician's Order SummaryJanelle Cabida SupnadNessuna valutazione finora