Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Taiji 24 Form - KellyDocumento18 pagineTaiji 24 Form - Kellyanattā100% (3)
- Science Checkpoint WorkbookDocumento130 pagineScience Checkpoint WorkbookAgung PambudionoNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Spanish VerbsDocumento26 pagineSpanish Verbstengohueva100% (1)
- Acls Manual PDFDocumento30 pagineAcls Manual PDFCyner Cruz100% (2)
- Aristotle On Soul and Soul - Parts' in SemenDocumento23 pagineAristotle On Soul and Soul - Parts' in SemenbrysonruNessuna valutazione finora
- Hygiene CareDocumento171 pagineHygiene CareCristina Benito100% (1)
- Bazaar Bargains Persona Peddling Peculiar Products with ProblemsDocumento10 pagineBazaar Bargains Persona Peddling Peculiar Products with ProblemsSekcerNessuna valutazione finora
- Standing Wealth: Pastoralist Livestock Production and Local Livelihoods in SudanDocumento80 pagineStanding Wealth: Pastoralist Livestock Production and Local Livelihoods in SudanFeinstein International CenterNessuna valutazione finora
- Bone and Parathyroid MetabolismDocumento6 pagineBone and Parathyroid MetabolismCyner CruzNessuna valutazione finora
- Community Health Nursing ExplainedDocumento28 pagineCommunity Health Nursing ExplainedCyner CruzNessuna valutazione finora
- Motor CortexDocumento2 pagineMotor CortexCyner CruzNessuna valutazione finora
- OB Dystocia Part II and IIIDocumento6 pagineOB Dystocia Part II and IIICyner CruzNessuna valutazione finora
- Community Health Nursing ExplainedDocumento28 pagineCommunity Health Nursing ExplainedCyner CruzNessuna valutazione finora
- Kang-Rizal ReportDocumento5 pagineKang-Rizal ReportCyner CruzNessuna valutazione finora
- Gynecoid Anthropoid Android Sonogram AccelerationDocumento137 pagineGynecoid Anthropoid Android Sonogram AccelerationCyner Cruz100% (1)
- Unit 1. Living Things: PRIMARY 3 / Natural Science Pedro Antonio López HernándezDocumento8 pagineUnit 1. Living Things: PRIMARY 3 / Natural Science Pedro Antonio López HernándezRJ RJNessuna valutazione finora
- 2015 Taufik Rekayasa Lampu Led Celup Untuk Perikanan Bagan ApungDocumento17 pagine2015 Taufik Rekayasa Lampu Led Celup Untuk Perikanan Bagan ApungKUD Mina KarotaNessuna valutazione finora
- Humane Stoat and Rodent Trap InstructionsDocumento4 pagineHumane Stoat and Rodent Trap InstructionsGina FelyaNessuna valutazione finora
- Living in The Environment: Sustaining Biodiversity: The Species ApproachDocumento73 pagineLiving in The Environment: Sustaining Biodiversity: The Species ApproachCE YMNessuna valutazione finora
- The Elements of Dance: Dance Concepts: SpaceDocumento2 pagineThe Elements of Dance: Dance Concepts: SpacePatrick LawagueNessuna valutazione finora
- Honey Bee Complaint As Community Policing For Scouting Against PCA Act, 1960: Restoring 5 FreedomsDocumento31 pagineHoney Bee Complaint As Community Policing For Scouting Against PCA Act, 1960: Restoring 5 FreedomsNaresh KadyanNessuna valutazione finora
- DolphinsDocumento2 pagineDolphinsdeepNessuna valutazione finora
- Unit 2BDocumento4 pagineUnit 2BGiang Nguyen Thi ThuNessuna valutazione finora
- Find the Odd Ball in 12 Identical Balls Using 3 WeighingsDocumento10 pagineFind the Odd Ball in 12 Identical Balls Using 3 WeighingsVijay SinghNessuna valutazione finora
- Coco film explores family, passion and truthDocumento1 paginaCoco film explores family, passion and truthFreetz TreeNessuna valutazione finora
- Spiders - Toxic or NotDocumento7 pagineSpiders - Toxic or NotKathy GreenNessuna valutazione finora
- Koala PowerpointDocumento9 pagineKoala Powerpointapi-237439124Nessuna valutazione finora
- Autonomic Pharmacology of the Eye/TITLEDocumento23 pagineAutonomic Pharmacology of the Eye/TITLERomaine-Ricardo FrancisNessuna valutazione finora
- B SC - H S - ZoologyDocumento49 pagineB SC - H S - Zoologyprince1900Nessuna valutazione finora
- Pearl Culture LectureDocumento28 paginePearl Culture LectureMahesh GKNessuna valutazione finora
- Harrell Horne Integrated School Pre-K Lesson PlanDocumento49 pagineHarrell Horne Integrated School Pre-K Lesson PlanMary Hope V. LazaroNessuna valutazione finora
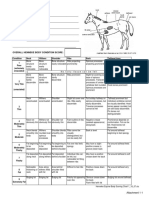
- Henneke BCS ChartDocumento1 paginaHenneke BCS ChartLaviniaMenicucciNessuna valutazione finora
- Triptico ADocumento1 paginaTriptico AalvaroNessuna valutazione finora
- Basic Human AnatomyDocumento6 pagineBasic Human AnatomySuman KumarNessuna valutazione finora
- Endocrine SystemDocumento8 pagineEndocrine SystemYenny AcostaNessuna valutazione finora
- Cuisine of SloveniaDocumento64 pagineCuisine of SloveniaKiran GadmaleNessuna valutazione finora
- Animal Bingo: ScalesDocumento3 pagineAnimal Bingo: ScalesjuliaNessuna valutazione finora
- Biopsychology 8E: John P.J. PinelDocumento37 pagineBiopsychology 8E: John P.J. PinelPhilip MercadoNessuna valutazione finora