Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Appendicitis
Caricato da
Jack GardnerCopyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Appendicitis
Caricato da
Jack GardnerCopyright:
Formati disponibili
GENERAL MEDICINE/CLINICAL POLICY
Clinical Policy: Critical Issues in the Evaluation and Management
of Emergency Department Patients With Suspected Appendicitis
From the American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Critical Issues
in the Evaluation and Management of Emergency Department Patients With Suspected Appendicitis:
John M. Howell, MD (Subcommittee Chair)
Orin L. Eddy, MD
Thomas W. Lukens, MD, PhD
Molly E. W. Thiessen, MD
Scott D. Weingart, MD
Wyatt W. Decker, MD (Committee Chair)
Members of the American College of Emergency Physicians Clinical Policies Committee (Oversight Committee):
Wyatt W. Decker, MD (Co-Chair 2006-2007, Chair 2007- Anthony M. Napoli, MD (EMRA Representative 2004-
2009) 2006)
Andy S. Jagoda, MD (Chair 2003-2006, Co-Chair 2006- Devorah J. Nazarian, MD
2007) AnnMarie Papa, RN, MSN, CEN, FAEN (ENA
Deborah B. Diercks, MD Representative 2007-2009)
Barry M. Diner, MD (Methodologist) Jim Richmann, RN, BS, MA(c), CEN (ENA Representative
Jonathan A. Edlow, MD 2006-2007)
Francis M. Fesmire, MD Scott M. Silvers, MD
John T. Finnell, II, MD, MSc (Liaison for Emergency Edward P. Sloan, MD, MPH
Medical Informatics Section 2004-2006) Molly E. W. Thiessen, MD (EMRA Representative 2006-
Steven A. Godwin, MD 2008)
Sigrid A. Hahn, MD Robert L. Wears, MD, MS (Methodologist)
Benjamin W. Hatten, MD (EMRA Representative 2008- Stephen J. Wolf, MD
2009) Cherri D. Hobgood, MD (Board Liaison 2004-2006)
John M. Howell, MD David C. Seaberg, MD, CPE (Board Liaison 2006-2009)
J. Stephen Huff, MD Rhonda R. Whitson, RHIA, Staff Liaison, Clinical Policies
Eric J. Lavonas, MD Committee and Subcommittees
Thomas W. Lukens, MD, PhD
Sharon E. Mace, MD Approved by the ACEP Board of Directors, October 2,
Donna L. Mason, RN, MS, CEN (ENA Representative 2009
2004-2006) Supported by the Emergency Nurses Association,
Edward Melnick, MD (EMRA Representative 2007-2008) November 3, 2009
Policy statements and clinical policies are the official policies of the American College of Emergency
Physicians and, as such, are not subject to the same peer review process as articles appearing in the print
journal. Policy statements and clinical policies of ACEP do not necessarily reflect the policies and beliefs
of Annals of Emergency Medicine and its editors.
0196-0644/$-see front matter
Copyright 2009 by the American College of Emergency Physicians.
doi:10.1016/j.annemergmed.2009.10.004
[Ann Emerg Med. 2010;55:71-116.]
Volume , . : January Annals of Emergency Medicine 71
Clinical Policy
ABSTRACT abdominal pain in its entirety, this policys scope is limited to 3
This clinical policy from the American College of Emergency questions:
Physicians is an update of a 2000 clinical policy on the 1. Can clinical findings be used to guide decisionmaking in the
evaluation and management of patients presenting with risk stratification of patients with possible appendicitis?
nontraumatic acute abdominal pain.1 A writing subcommittee 2. In adult patients with suspected acute appendicitis who are
reviewed the literature to derive evidence-based recommendations undergoing a CT scan, what is the role of contrast?
to help clinicians answer the following critical questions: (1) 3. In children with suspected acute appendicitis who undergo
Can clinical findings be used to guide decisionmaking in the diagnostic imaging, what are the roles of CT and ultrasound
risk stratification of patients with possible appendicitis? (2) In in diagnosing acute appendicitis?
adult patients with suspected acute appendicitis who are
undergoing a computed tomography scan, what is the role of METHODOLOGY
contrast? (3) In children with suspected acute appendicitis who This clinical policy was created after careful review and
undergo diagnostic imaging, what are the roles of computed critical analysis of the medical literature. Multiple searches of
tomography and ultrasound in diagnosing acute appendicitis? MEDLINE and the Cochrane database were performed.
Evidence was graded and recommendations were given based on Specific key words/phrases used in the searches are identified
the strength of the available data in the medical literature. under each critical question. To update the 2000 American
College of Emergency Physicians (ACEP) policy, all searches
were limited to English-language sources, human studies, and to
INTRODUCTION articles published from January 2000 to March 2007.
Abdominal pain is a high-volume, high-risk chief complaint. Additional articles were reviewed from the bibliography of
In 2005, patients with abdominal pain composed 6.8% of 115 articles cited and from published textbooks and review articles.
million annual emergency department (ED) visits.2 Ten percent Subcommittee members supplied articles from their own files,
of closed malpractice claims for emergency physicians involve and more recent articles identified during the process were also
the missed diagnosis of abdominal pain.3 Among children included.
between 6 and 17 years of age, appendicitis is the second most The reasons for developing clinical policies in emergency
common cause of malpractice litigation against emergency medicine and the approaches used in their development have
physicians.4 The diagnosis of appendicitis can be challenging been enumerated.6 This policy is a product of the ACEP clinical
even in the most experienced of clinical hands. policy development process, including expert review, and is
Despite the increasing utilization of computed tomography based on the existing literature; when literature was not
(CT) in patients with possible appendicitis, such widespread use available, consensus of emergency physicians was used. Expert
may be unnecessary. Clinical indicators (eg, signs, symptoms, review comments were received from individual emergency
laboratory tests) exist that might identify patients who require physicians and from individual members of the American
abdominal CT to diagnose acute appendicitis. Such indicators Academy of Pediatrics, the American College of Radiology, the
could facilitate the early identification of ED patients who do Society for Academic Emergency Medicine, the Society for
and do not require CT, but are such strategies effective? Pediatric Radiology, ACEPs Pediatric Emergency Medicine
Once the decision is made to image, performing a CT may Section, and ACEPs Emergency Ultrasound Section. Their
or may not involve the use of contrast. If contrast is used, does responses were used to further refine and enhance this policy;
it increase diagnostic performance in a clinically meaningful however, their responses do not imply endorsement of this
way? In children, some clinicians use ultrasound before or in clinical policy. Clinical policies are scheduled for revision every
lieu of CT to diagnose appendicitis. Although ultrasound does 3 years; however, interim reviews are conducted when
not involve ionizing radiation or the risks associated with technology or the practice environment changes significantly.
contrast, the accuracy of either a positive or negative ultrasound All articles used in the formulation of this clinical policy were
result merits discussion. graded by at least 2 subcommittee members for strength of
Not every patient with possible appendicitis needs evidence and classified by the subcommittee members into 3
abdominal imaging. Although this clinical policy addresses classes of evidence on the basis of the design of the study, with
diagnostic studies for appendicitis, not all patients with possible design 1 representing the strongest evidence and design 3
appendicitis require diagnostic tests. For example, patients with representing the weakest evidence for therapeutic, diagnostic,
very low clinical suspicion for appendicitis may be discharged and prognostic clinical reports, respectively (Appendix A).
with minimal or no testing. Similarly, patients with high clinical Articles were then graded on 6 dimensions thought to be most
suspicion for appendicitis may be referred to a surgeon, with relevant to the development of a clinical guideline: blinded
minimal or no testing.5 If the clinical presentation warrants, a versus nonblinded outcome assessment, blinded or randomized
surgical consultant should be notified as early as is clinically allocation, direct or indirect outcome measures (reliability and
warranted. validity), biases (eg, selection, detection, transfer), external
This clinical policy addresses evidence-based questions validity (ie, generalizability), and sufficient sample size. Articles
framed around these issues. Rather than approach the topic of received a final grade (Class I, II, III) on the basis of a
72 Annals of Emergency Medicine Volume , . : January
Clinical Policy
predetermined formula, taking into account design and quality answer a critical question. When the medical literature does
of study (Appendix B). Articles with fatal flaws were given an not contain enough quality information to answer a critical
X grade and not used in formulating recommendations in this question, the members of the Clinical Policies Committee
policy. Evidence grading was done with respect to the specific believe that it is equally important to alert emergency
data being extracted and the specific critical question being physicians to this fact.
reviewed. Thus, the level of evidence for any one study may vary Recommendations offered in this policy are not intended to
according to the question, and it is possible for a single article to represent the only diagnostic and management options that the
receive different levels of grading as different critical questions emergency physician should consider. ACEP clearly recognizes
are answered. Question-specific level of evidence grading may be the importance of the individual physicians judgment. Rather,
found in the Evidentiary Table included at the end of this this guideline defines for the physician those strategies for which
policy. medical literature exists to provide support for answers to the
Clinical findings and strength of recommendations regarding crucial questions addressed in this policy.
patient management were then made according to the following Scope of Application. This guideline is intended for
criteria: physicians working in hospital-based EDs.
Level A recommendations. Generally accepted principles for Inclusion Criteria. This guideline is intended for patients
patient management that reflect a high degree of clinical presenting to the ED with acute, nontraumatic abdominal pain
certainty (ie, based on strength of evidence Class I or and possible or suspected appendicitis.
overwhelming evidence from strength of evidence Class II Exclusion Criteria. This guideline is not intended to
studies that directly address all of the issues). address the care of patients with trauma-related abdominal pain,
Level B recommendations. Recommendations for patient or pregnant patients.
management that may identify a particular strategy or range of
management strategies that reflect moderate clinical certainty
(ie, based on strength of evidence Class II studies that directly CRITICAL QUESTIONS
address the issue, decision analysis that directly addresses the 1. Can clinical findings be used to guide decisionmaking
issue, or strong consensus of strength of evidence Class III in the risk stratification of patients with possible
studies). appendicitis?
Level C recommendations. Other strategies for patient
management that are based on preliminary, inconclusive, or Patient Management Recommendations
conflicting evidence, or in the absence of any published Level A recommendations. None specified.
literature, based on panel consensus. Level B recommendations. In patients with suspected acute
There are certain circumstances in which the appendicitis, use clinical findings (ie, signs and symptoms) to
recommendations stemming from a body of evidence should risk-stratify patients and guide decisions about further testing
not be rated as highly as the individual studies on which they (eg, no further testing, laboratory tests, and/or imaging studies),
are based. Factors such as heterogeneity of results, uncertainty and management (eg, discharge, observation, and/or surgical
about effect magnitude and consequences, strength of prior consultation).
beliefs, and publication bias, among others, might lead to such a Level C recommendations. None specified.
downgrading of recommendations.
When possible, clinically oriented statistics (ie, likelihood Key words/phrases for literature searches: appendicitis,
ratios, odds ratios, risk ratios, and number needed to treat) will abdominal pain, clinical indicators, clinical predictors,
be presented to help the reader better understand how the prediction rule, probability, sensitivity and specificity or
results can be used with the patient and will be given priority predictive value of tests or ROC curve, diagnosis, differential,
over simple descriptive statistics (eg, sensitivity, specificity, and decisionmaking, decision support techniques, diagnostic errors,
predictive values). The former allow the reader to interpret missed diagnoses, computed tomography, and variations and
study results taking into consideration probability of disease. combinations of the key words/phrases.
For a more thorough explanation of these statistical Whereas the diagnosis of appendicitis is often
methodologies, see Appendix C. straightforward, many patients present with early or atypical
This policy is not intended to be a complete manual on the signs and symptoms. Further, laboratory test results may be
evaluation and management of patients with nontraumatic normal in the setting of appendicitis. We reviewed the literature
acute abdominal pain but rather a focused examination of to determine which clinical findings, if any, risk-stratify patients
critical issues that have particular relevance to the current with suspected appendicitis and suggest the need for either a
practice of emergency medicine. radiologic procedure or surgery.
It is the goal of the Clinical Policies Committee to For the purposes of this publication, missed appendicitis is
provide an evidence-based recommendation when the considered a false-negative clinical evaluation, and the removal of a
medical literature provides enough quality information to normal appendix is considered a false-positive clinical evaluation.
Volume , . : January Annals of Emergency Medicine 73
Clinical Policy
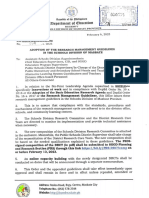
History and Physical Examination Table 1. Alvarado score in acute appendicitis.
In a meta-analysis of approximately 4,000 patients (Class II), Value
right lower quadrant abdominal pain was the most useful
Symptoms Migration 1
clinical finding in suspected appendicitis (positive likelihood Anorexia-acetone (in the urine) 1
ratio 95% confidence interval [CI] 7.31 to 8.46 and a negative Nausea-vomiting 1
likelihood ratio 95% CI 0 to 0.28).7 The authors only reported Signs Tenderness in right lower quadrant 2
95% CI because the included studies were heterogeneous.7 In a Rebound pain 1
separate meta-analysis, Andersson8 found that pain migration Elevation of temperature (37.3C 1
measured orally)
(positive likelihood ratio 2.06, 95% CI 1.63 to 2.60; and
negative likelihood ratio 0.42, 95% CI 0.40 to 0.69) and pain Laboratory Leukocytosis (10,000/mm3) 2
Shift to the left (75% neutrophils) 1
progression (positive likelihood ratio 1.39, 95% CI 1.29 to
Total score 10
1.50; and negative likelihood ratio 0.46, 95% CI 0.27 to 0.77)
Score
were less helpful. Two Class III studies found that right lower 1-4 Appendicitis unlikely
quadrant tenderness had positive likelihood ratios of 2.3 and 1.1 5-6 Appendicitis possible
and negative likelihood ratios of 0 and 0.1.9,10 Rigidity on 7-8 Appendicitis probable
abdominal examination carried a positive likelihood ratio of 3.8. 9-10 Appendicitis very probable
Anorexia, tenderness on rectal examination, guarding, fever, and Adapted from Alvarado A. A practical score for the early diagnosis of acute ap-
percussion tenderness in the right lower quadrant all had pendicitis. Ann Emerg Med. 1986;15:557-564 with permission from Elsevier.
positive likelihood ratios below 2.9.7,8
Laboratory Tests retrospectively from patients hospitalized with suspected
Although the total WBC count is frequently used in the appendicitis. The Alvarado score combines patient symptoms,
diagnostic evaluation of acute appendicitis, when used alone it is physical examination results, and laboratory values to assign a
not a consistent predictor. Cardall et al11 demonstrated a score from 0 to 10.
positive likelihood ratio for an elevated WBC count (10,000/ Theoretically, higher Alvarado scores are associated with a
mm3) of 1.59 and a negative likelihood ratio of 0.46. In the higher likelihood of appendicitis and lower scores with a lower
meta-analysis by Andersson,8 the positive likelihood ratio of an likelihood of appendicitis. Whether the Alvarado score can
elevated WBC count (10,000/mm3) for appendicitis was 2.47 reliably predict the need for CT is debatable. In a Class III
(95% CI 2.06 to 2.95) and the negative likelihood ratio was study, McKay and Shepherd15 reviewed 150 charts to develop
0.25 (95% CI 0.18 to 0.36). The positive likelihood ratio was guidelines for CT scanning based on Alvarado scoring. Five
3.47 (95% CI 1.6 to 7.8) in those patients with a WBC count percent of patients with scores of 3 or less had appendicitis,
greater than 15,000/mm3.8 36% of patients with scores between 4 and 6 had appendicitis,
In a Class III study, Kessler et al12 found that an elevated WBC and 78% of patients with scores of 7 or higher had appendicitis.
count (10,000/mm3) carried a positive likelihood ratio of 2.7 and The authors concluded that patients with scores of 3 or less
a negative likelihood ratio of 0.5. Birchley13 found similar results should not have CT (2 patients with appendicitis would have
when evaluating the WBC count in a small single-surgeon series. been missed in their series), those with scores between 4 and 6
Whereas neither the WBC count nor the C-reactive protein should have CT, and those with scores 7 or higher would
level consistently diagnoses or excludes appendicitis when used benefit from surgical consultation before CT. Chan et al,16 in a
alone, the combination of C-reactive protein and WBC count is Class III study, found that no patients with Alvarado scores
more helpful.8 For a C-reactive protein level of 10 mg/L, below 5 had appendicitis.
Andersson8 identified a positive likelihood ratio of 4.24 (95% In 2 other studies, a low Alvarado score did not reliably exclude
CI 1.16 to 15.53) and a negative likelihood ratio of 0.11 (95% appendicitis or the need for CT. In a Class III study, Gwynn9
CI 0.05 to 0.25) for acute appendicitis. However, in this same found that 12 (8.4%) of 143 subjects with appendicitis had
meta-analysis, the negative likelihood ratio for the combination Alvarado scores below 5. Patients in extremes of age (60 to 80 and
of a WBC count of 10,000/mm3 and a C-reactive protein of 8 0 to 10 years of age) were misdiagnosed more frequently. In a small
mg/L was 0.03 (95% CI 0.0 to 0.14). The positive likelihood Class III study, Yildirim et al17 found that 72% of patients with
ratio for the combination of both of these laboratory results was Alvarado scores between 1 and 4 ultimately had appendicitis,
23.32 (95% CI 6.87 to 84.79). according to CT results and subsequent surgery. The authors
recommended imaging even patients with low Alvarado scores.
The Alvarado Score
Combining various signs and symptoms into a scoring system Pediatric Considerations
may be more useful in predicting the presence or absence of In a Class II prospective cohort study, Kharbanda et al18
appendicitis. The Alvarado score, originally described in 1986, identified 5 historical, physical examination, and laboratory
is the most widely reported scoring system for acute findings that are significantly associated with pediatric
appendicitis14 (Table 1). The score was developed appendicitis. The authors used logistic regression to identify
74 Annals of Emergency Medicine Volume , . : January
Clinical Policy
nausea, a history of focal right lower quadrant pain, difficulty contrast highlights inflammation in the wall of the appendix
walking, rebound tenderness, and an absolute neutrophil count and in the tissue around the appendix.22,23 Enteric contrast
of greater than 6,750/mm3 as significantly associated with acute helps differentiate the appendix from surrounding
appendicitis.18 When these variables were combined into a structures.24,25 Enteric and IV contrast may be more helpful in
scoring system and applied to a validation cohort, the scoring thin patients with low body mass index who lack sufficient
system resulted in a negative likelihood ratio of 0.058 (95% CI mesenteric fat to demonstrate periappendiceal fat stranding that
0.008 to 0.41). is associated with appendicitis.26-28 Enteric and IV contrast also
In a Class III study, Wang et al19 evaluated the diagnostic help identify conditions other than acute appendicitis (eg,
performance of selected blood tests in children presenting to the diverticulitis, inflammatory bowel disease, cancer).22,29,30
ED with possible appendicitis. The authors defined an elevated Contrast has disadvantages. Oral contrast requires time to
WBC count and a left shift based on age-defined normal values. administer, requires time to transit the bowel, and may be
For both an elevated WBC count and a left shift, the positive difficult to tolerate for patients with abdominal pain and
likelihood ratio was 9.8. For either an elevated WBC count or a
vomiting. Rectal contrast requires less time to administer than
left shift, the negative likelihood ratio was 0.26. In contrast, the
oral contrast but may be uncomfortable and unpleasant. IV
diagnostic performances of an elevated WBC count (positive
contrast may lead to serious allergic reactions and renal failure.
likelihood ratio 3.4; negative likelihood ratio 0.41) and a left
Contrast also adds to cost.31 Increased sensitivity of newer-
shift (positive likelihood ratio 5.9; negative likelihood ratio
generation multislice CT scanners may improve diagnostic
0.45) individually were not as strong. The authors of this study
did not disclose a criterion standard for the diagnosis or accuracy, obviating the need for contrast.
exclusion of acute appendicitis. Multiple investigators have studied CT of the abdomen and
In a Class III prospective study, van den Broek et al20 found pelvis for the evaluation of acute appendicitis (Table 2). Most of
that temperature greater than 38C, a WBC count of 10,100/ these studies evaluate a single CT technique (eg, noncontrast
mm3 or greater, and rebound tenderness were significantly CT, CT with oral contrast, CT with rectal contrast, CT with IV
associated with pediatric appendicitis. Using these factors in a contrast, CT with some combination of contrast types). In the
scoring system, they created a prediction rule that resulted in a majority of these studies, CT performs reasonably well,
1% missed appendicitis rate and a 9% negative appendectomy regardless of whether or not contrast is used.22,26,27,31-49 When
rate. these studies are compared, it appears that the improvement in
In a retrospective study, Klein et al21 identified guarding and diagnostic accuracy achieved by the addition of IV or enteric
temperature greater than 38.4C as predictive of appendicitis in contrast is small.
girls 5 to 12 years of age, and tenderness and vomiting as To determine the utility of oral contrast, Anderson et al50
predictive in boys 5 to 12 years of age. In boys older than 12 performed a systematic review of 23 prospective and
years, guarding and anorexia were predictive of appendicitis. In retrospective reports on CT for suspected appendicitis. They
contrast to the studies by Kharbanda et al18 and van den Broek reported the following weighted sensitivities and specificities:
et al,20 Klein et al21 found that adding WBC count to other noncontrast CT 93% and 98%, CT with oral and IV contrast
clinical factors decreased diagnostic performance. 93% and 93%, and CT with rectal contrast 97% and 97%. The
2. In adult patients with suspected acute appendicitis who authors concluded that oral contrast does not improve the
are undergoing a CT scan, what is the role of contrast? accuracy of CT for the diagnosis of acute appendicitis.
The majority of publications concerning CT for the
Patient Management Recommendations evaluation of acute appendicitis report on a single CT
Level A recommendations. None specified. technique. Comparing the available studies of individual CT
Level B recommendations. In adult patients undergoing a techniques is problematic. Study design varies significantly
CT scan for suspected appendicitis, perform abdominal and among the articles: setting (university versus community), study
pelvic CT scan with or without contrast (intravenous [IV], oral, population (radiology series versus surgical series versus ED
or rectal). The addition of IV and oral contrast may increase the population), level of radiologist training and experience,
sensitivity of the CT scan for the diagnosis of appendicitis. inclusion criteria (all patients with suspected appendicitis versus
Level C recommendations. None specified. those with equivocal presentations), CT slice type (helical versus
Key words/phrases for literature searches: appendicitis, conventional) and slice thickness (range 2.5 mm to 10 mm),
computed tomography, contrast, diagnosis, sensitivity, enteric contrast protocol (type of oral contrast: barium,
specificity, and variations and combinations of the key words/ meglumine diatrizoate, diatrizoate sodium, or meglumine
phrases. ioxitalamate), and contrast transit time (oral contrast transit
Performing abdominal and pelvic CT without enteric or IV times ranged from 40 minutes to longer than 2 hours).
contrast for the evaluation of patients with suspected acute To determine which CT technique is superior, CT
appendicitis is appealing for its speed and simplicity. Whether techniques should be compared in a prospective, randomized
contrast provides a diagnostic advantage has been debated. IV trial. Only 3 studies have compared CT techniques head to
Volume , . : January Annals of Emergency Medicine 75
Clinical Policy
Table 2. Diagnostic accuracy of CT for diagnosing acute appendicitis in adults.
CT Technique Study No. Pts. Prevalence % Positive LR Negative LR Sensitivity % Specificity % Class
27
No contrast Lane et al 109 38 30 0.10 90 97 I
int Hof et al33 103 85 Undefined 0.05 95 100 I
Lane et al34 300 38 96 0.04 96 99 I
Ege et al26 296 36 48 0.04 96 98 II
Malone et al31 211 36 29 0.13 87 97 II
Hershko et al32* 70 41 6.4 0.12 90 86 II
Cakirer et al35 130 72 12 0.05 95 92 II
Horton et al36 49 76 Undefined 0.03 97 100 II
Tamburrini et al23 404 20 22 0.10 90 96 III
45
DIppolito et al 52 85 Undefined 0.09 91 100 III
Morris et al46 129 30 9.8 0.13 88 91 III
Oral and IV Jacobs et al22* 210 22 18 0.10 91 95 I
contrast Hershko et al32* 84 51 9 0 100 89 II
Balthazar et al37 100 64 5.8 0.02 98 83 II
Hershko et al38 198 38 11 0.10 91 92 II
Kamel et al39 100 24 Undefined 0.40 96 100 II
Schuler et al40 97 52 49 0.02 98 98 II
Ujiki et al30 110 25 8.2 0.11 90 89 III
Rectal Rao et al41 100 53 49 0.02 98 98 I
contrast Hershko et al32* 78 50 19 0.07 93 95 II
Pickuth and 120 78 8.6 0.06 95 89 II
Spielmann42
Walker et al43 65 54 Undefined 0.06 94 100 II
44
Wong et al 50 74 12 0.05 95 92 II
Mittal et al51* 39 92 Undefined 0.12 88 100 III
Oral contrast Jacobs et al22* 210 22 13 0.26 76 94 I
Wijetunga et al28 100 30 31 0.07 93 97 I
Rectal, oral, Mittal et al51* 52 85 6.9 0.04 97 86 III
and IV
contrast
Rectal and IV Naffaa et al47 75 47 .10 0 100 90 II
contrast
Rectal/-oral Funaki et al24 100 30 16 0.03 97 94 II
contrast
Oral and rectal Rao et al48 100 56 20 0 100 95 I
contrast
IV contrast Mun et al49 173 32 33 0 100 97 III
Pts, patients; LR, likelihood ratio.
*Article appears in chart more than once because 2 or more techniques were studied.
Analysis does not include inconclusive results.
head.22,32,51 Two of these 3 studies suggest that the addition of contrast; CT with oral and IV contrast showed a trend
contrast does improve the diagnostic performance of CT.22,32 toward increased sensitivity over CT without contrast. In
this Class II study, Hershko et al32 randomized 232
CT With Oral and IV Contrast Versus CT With Rectal consecutive patients with suspected appendicitis to one of 3
Contrast Versus Noncontrast CT protocols: 70 patients had CT without contrast, 78 patients
Hershko et al32 published the only prospective had CT with rectal contrast, and 84 patients had CT with
randomized study comparing 3 different contrast protocols. oral and IV contrast. CT with rectal contrast and CT with
CT with oral and IV contrast, and CT with rectal contrast oral and IV contrast were both more accurate than CT
were each more accurate than CT without contrast; CT with without contrast: 94%, 94%, and 70%, respectively
oral and IV contrast was more sensitive than CT with rectal (P0.05). CT with oral and IV contrast was more sensitive
76 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Table 3. Diagnostic accuracy of ultrasound in diagnosing acute appendicitis in children.
Disease
Reference No. Subjects Prevalence, % Positive LR Negative LR Sensitivity, % Specificity, % Class
Baldisserotto and 425 47 49.5 0.01 99 (95% CI 98 (95% CI II
Marchiori55 97-100) 97-99)
Kaiser et al56 283 41 17.2 0.14 86 95 II
Chang et al57 40 75 8.7 0.14 87 90 III
Dilley et al58 587 86 17.8 0.12 89 95 III
Lowe et al59 76 33 8.3 0 100 88 III
Sivit et al60 315 26 11.1 0.2 78 93 III
Teo et al61 129 22 31 0.07 93 97 III
Ranges 40-587 subjects 22-86 8.3-49.5 0-0.2 78-100 88-98 II-III
than CT with rectal contrast, 100% (negative likelihood contrast. In a Class III study, Tamburrini et al23 reported a CT
ratio 0) versus 93% (negative likelihood ratio 0.07) protocol with selective use of contrast. Patients with suspected
(P0.05). CT with oral and IV contrast was observed to appendicitis were first evaluated with noncontrast CT of the
differ from CT without contrast with sensitivities of 100% abdomen and pelvis. Patients with inconclusive results were
(negative likelihood ratio 0) versus 90% (negative likelihood rescanned with contrast, the type of contrast determined on a
ratio 0.12), respectively; however, this difference did not case-by-case basis by the interpreting radiologist. The authors
achieve statistical significance. performed a retrospective review of 536 patients undergoing
this protocol. Noncontrast CT was conclusive in 404 (75%)
CT With Oral Contrast Versus CT With Oral and IV Contrast patients and inconclusive in 132 (25%). Repeat CT was
In a Class I study, Jacobs et al22 prospectively compared 2 performed with some type of contrast in 126 (24%) patients.
different contrast protocols and concluded that IV contrast
improved the sensitivity of CT. In a case-crossover-design trial that 3. In children with suspected acute appendicitis who
included 210 subjects, each patient had focused appendiceal CT undergo diagnostic imaging, what are the roles of CT and
with only oral contrast, followed by nonfocused abdomen and ultrasound in diagnosing acute appendicitis?
pelvis CT with oral and IV contrast. The sensitivity of the
nonfocused abdomen and pelvis CT with oral and IV contrast was Patient Management Recommendations
91% (negative likelihood ratio 0.1), whereas the sensitivity of the Level A recommendations. None specified.
focused appendiceal CT with oral contrast was 76% (negative Level B recommendations.
likelihood ratio 0.26). The authors attributed the higher sensitivity 1. In children, use ultrasound to confirm acute appendicitis
of the nonfocused abdomen and pelvis CT to the use of IV but not to definitively exclude acute appendicitis.
contrast; they believed that IV contrast improved the ability of the 2. In children, use an abdominal and pelvic CT to confirm or
radiologist to identify an inflamed appendix. exclude acute appendicitis.
Level C recommendations. Given the concern over
CT With Oral, Rectal, and IV Contrast Versus CT With Rectal
exposing children to ionizing radiation, consider using
Contrast
ultrasound as the initial imaging modality. In cases in which the
In a Class III study, Mittal et al51 compared the accuracy of
diagnosis remains uncertain after ultrasound, CT may be
2 contrast protocols. The authors prospectively compared CT of
performed.
the abdomen and pelvis with oral, rectal, and IV contrast to
focused CT of the lower abdomen and pelvis with rectal Key words/phrases for literature searches: children,
contrast only. They found that CT with oral, rectal, and IV appendicitis, computed tomography, ultrasound, radiation,
contrast had a sensitivity of 97% and specificity of 86% diagnosis, abdominal pain, sensitivity, specificity, and variations
(negative likelihood ratio 0.04 and positive likelihood ratio 6.9), and combinations of the key words/phrases.
whereas CT with rectal contrast had a sensitivity of only 88% The diagnosis of acute appendicitis is challenging in the
and a specificity of 100% (negative likelihood ratio 0.12 and an pediatric population, particularly among infants and toddlers.
undefined positive likelihood ratio). The authors did not report Missed or delayed diagnosis may result in perforation.
whether these differences were statistically significant. Perforation rates for the pediatric population range from 17%
to 57%,52 which may cause longer hospital stays, bowel
Inconclusive Results and Noncontrast CT obstruction, and sepsis.53,54
Noncontrast CT may produce inconclusive results. In the CT has been advocated because it is an accurate diagnostic
previously described study by Hershko et al,32 14 (20%) of 70 modality. However, CT is expensive and often requires contrast.
patients in the CT without contrast group had inconclusive CT CT also exposes the patient to ionizing radiation. Ultrasound
results. Nine (13%) patients had repeat CTs with oral and IV has been advocated because it is fast, well tolerated, and safe.
Volume , . : January Annals of Emergency Medicine 77
Clinical Policy
Table 4. Diagnostic accuracy of CT in diagnosing acute appendicitis in children.
No. Disease
Reference Subjects Prevalence, % Contrast Type Positive LR Negative LR Sensitivity, % Specificity, % Class
59
Lowe et al 72 33 None Undefined 0.03 97 100 II
Kaiser et al62 306 42 Either no contrast or No contrast: 6.6; No contrast: No contrast: No contrast: II
just IV contrast IV contrast: 16 0.38; 66; 90;
IV contrast: IV contrast: IV contrast:
0.04 96 94
Sivit et al60 153 26 IV in 145/153 (95%), 13.6 0.05 95 93 III
and oral or rectal
in 151/153 (99%)
Acosta et al63 94 16 Rectal (alone) 50 0 100 (95% CI 98 (95% CI III
66-100) 88-100)
Hoecker and 112 38 None 14.7 0.13 88 (95% CI 94 (95% CI III
Billman64 76-95) 95-98)
Mullins et al65 199 33 Rectal (alone) 97 0.03 97 99 III
Kharbanda et 416 40 Either IV alone or IV IV alone: 11.6; IV IV alone: IV alone: IV alone: III
al66 and rectal and rectal: 7.1 0.08; IV 93 (95% CI 92 (95% CI
and rectal: 84-97); IV 85-96); IV
0.09 and rectal: and rectal:
92 (95% CI 87 (95% CI
85-97) 79-92)
Ranges 72-416 16-42 No contrast: 6.6- No contrast: No contrast: No contrast: II-III
undefined; 0.03-0.38; 66-97; 90-100;
rectal contrast: rectal rectal rectal
50-97; IV contrast: contrast: contrast:
contrast: 11.6- 0-0.03; IV 97-100; IV 98-99; IV
16; IV and contrast: contrast: contrast:
rectal contrast: 0.04-0.08; 93-96; IV 92-94; IV
7.1; all results: IV and and rectal and rectal
6.6-undefined rectal contrast: contrast:
contrast: 92; all 87; all
0.09; all results: results:
results: 66-100 87-100
0-0.38
Diagnostic Accuracy of Ultrasound the ultrasound technique used by Baldisserotto and
Ultrasound may be used to evaluate children for appendicitis Marchiori55 did not assess compressibility of the appendix (a
and does not involve ionizing radiation exposure. Diagnostic diagnostic criterion in most studies). In the study by Kaiser
criteria for appendicitis are an appendix greater than 6 mm in et al,56 ultrasound results were interpreted by pediatric
diameter, a noncompressible appendix, and appendiceal surgeons and surgical residents, not radiologists. This limited
tenderness. However, the appendix may be obscured (by bowel the studys generalizability.
gas) or difficult to find (eg, retrocecal position). The 7 studies Of the 5 Class III ultrasound studies, 3 are prospective57,60,61
that evaluate the diagnostic accuracy of ultrasound in pediatric and 2 are retrospective.58,59 These Class III studies report
appendicitis (Table 3) support the idea that ultrasound is better positive likelihood ratios from 8.3 to 31 and negative
at positively identifying appendicitis than excluding it with a likelihood ratios from 0 to 0.2. Of these prospective Class III
negative or equivocal result.55-61 For example, although 3 of the studies, the study by Chang et al57 had a small sample size
7 studies listed in Table 3 report negative likelihood ratios for (40 subjects). Two of the studies did not adequately identify
ultrasound less than 0.1,55,59,61 5 of these 7 studies report or describe the outpatient follow-up of subjects with negative
positive likelihood ratios greater than 10.55,56,58,60,61 study results.60,61 The ultrasound outcomes from the study
There are no Class I studies evaluating ultrasound for by Lowe et al59 were taken from the retrospective control
acute appendicitis in children. There are 2 Class II studies arm of a prospective study. Lowe et al59 also did not describe
evaluating ultrasound in pediatric appendicitis.55,56 Both the duration of outpatient follow-up of subjects with
studies are prospective evaluations that report positive negative study results, and their study had a relatively small
likelihood ratios from 17.2 to 49.5 and negative likelihood sample size (76 subjects). Dilley et al58 did not describe a
ratios from 0.01 to 0.14. Baldisserotto and Marchiori55 was criterion standard for outpatient follow-up of negative
limited by lack of operator (ie, radiologist) blinding. Also, ultrasound results.
78 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Diagnostic Accuracy of Abdominal and Pelvic CT Ionizing Radiation and CT
According to Class II and III evidence, CT is better than There are no prospective studies that prove a link between
ultrasound at confirming and excluding appendicitis. Seven CT and cancer in children. However, 2 Class III unstructured
studies evaluated abdominal CT in diagnosing pediatric reviews argue that, because ionizing radiation at high doses (eg,
appendicitis59,60,62-66 (Table 4). Of the 7 studies that atomic bomb) is associated with cancer, and this high-dose risk
evaluated CT for pediatric appendicitis, all study arms that may proceed in a predictable fashion with dose, there may be a
involved the use of some type of contrast reported negative similar but small risk to children receiving diagnostic radiologic
likelihood ratios less than 0.1, and all but one study66 procedures (eg, CT).67,68
involving some type of contrast reported positive likelihood Another Class III article develops the argument supporting
ratios greater than 10. All studies except one66 reported the risk of ionizing radiation from CT in a slightly different
specificities of 90% or greater. Specifically, 2 Class III studies way.69 Brenner and Hall69 first present data that about 30% of
of rectal contrast only reported positive likelihood ratios patients who receive an abdominal and pelvic CT also receive at
from 50 to 97 and negative likelihood ratios from 0 to 0.03 least 3 such CT scans in the course of their care. The authors
for acute appendicitis.63,65 then present data that atomic bomb survivors who received 50
Four of these studies were prospective59,60,62,63 and 3 were to 150 mSv* of radiation had a small increase in cancer risk.
retrospective.64,65,66 Limitations of the articles by Lowe et al59 Two to 3 abdominal/pelvic CT scans expose patients to a level
and Sivit et al60 are discussed under the ultrasound section. CT of millisieverts similar to that of some atomic bomb survivors
outcomes from the study by Lowe et al59 were graded as Class II who developed cancer. Extrapolating backwards, the authors
because the data were collected prospectively. estimate the lifetime attributable risk of all cancers from 1
The Class II 2004 study by Kaiser et al62 was based on CT abdominal and pelvic CT to be 0.14% in neonates and
scans from their 2002 study. These scans were reread by 3 approximately 0.06% in adults. Children have a higher risk of
radiologists who were blinded to patient outcomes and developing cancer after radiation exposure because they have
compared with outcomes from the 2002 study. The prospective more years to develop those cancers and are more radiosensitive
study by Acosta et al63 was limited by sample size (43 children (children have more actively dividing cells than adults).
included in outcomes calculations), generalizability (excluded In an effort to limit ionizing radiation exposure, some centers
children younger than 6 years), and potential bias (CT scans are using a staged approach by initially using ultrasound, and
read by 1 radiologist). In 2007, Kharbanda et al66 then using CT either to confirm or exclude the diagnosis in
retrospectively studied 416 children who received a CT with selected cases.70,71 At this writing, this strategy has not been
either IV or IV and rectal contrast. Although Kharbanda et al66 definitively validated in prospective studies.
collected data retrospectively, the study was designed to occur
throughout 2 consecutive study periods, during which children Future Areas of Research
received one of the 2 CT techniques. In the study by Hoecker The following are suggestions for future research:
and Billman,64 which was retrospective, 15 of 112 children were 1. A prospective comparison of CT with no contrast, IV
lost to follow-up. Mullins et al65 conducted a retrospective contrast alone, and oral and IV contrast (for appendicitis),
study that had possible selection bias; children chosen for study using the newest CT technology. This study could be done
may have been more clinically straightforward. in both adult and pediatric populations.
We found no prospective, randomized comparisons of 2. An analysis of a Bayesian approach using ultrasound to
ultrasound and CT for pediatric appendicitis. Three studies diagnose appendicitis in children. For example, in a child
attempted to compare CT and ultrasound.56,59,60 The Sivit et with low pretest clinical suspicion of appendicitis, does a
al60 study was not randomized, Lowe et al59 used a historical negative or nondiagnostic ultrasound result suffice to
control group, and Kaiser et al56 compared CT with ultrasound exclude the diagnosis?
followed by CT. 3. An analysis of clinical factors using recursive partitioning to
The value of using CT with oral and IV contrast to diagnose determine whether combinations of history, physical
appendicitis in children remains unclear. We found no direct examination, and laboratory results can help diagnose or
evaluation of the diagnostic performance of oral and IV contrast exclude appendicitis. For example, does a negative WBC
alone for appendicitis in children. Nevertheless, some clinicians count and C-reactive protein result, combined with other
use oral and IV contrast to diagnose pediatric appendicitis clinical factors, exclude acute appendicitis?
according to the adult literature (discussed under critical 4. Research protocols that focus on techniques for limiting
question 2 about the role of contrast in CT for acute ionizing radiation exposure from CT used to diagnose
appendicitis in adults). Most children are smaller than adults appendicitis.
and may have different peritoneal fat distributions. The 5. A study of the role of MRI in diagnosing appendicitis.
question of whether or not adult outcomes (for CT in
appendicitis) can be applied to children of all ages and sizes *Millisieverts are the measure of radiation dose to organs, and this
remains unanswered. measurement is generally used in risk assessments of radiation.
Volume , . : January Annals of Emergency Medicine 79
Clinical Policy
Relevant industry relationships of subcommittee 18. Kharbanda AB, Taylor GA, Fishman SJ, et al. A clinical decision
members: There were no relevant industry relationships rule to identify children at low risk for appendicitis. Pediatrics.
2005;116:709-716.
disclosed by the subcommittee members. 19. Wang LT, Prentiss KA, Simon JZ, et al. The use of white blood
Relevant industry relationships are those relationships cell count and left shift in the diagnosis of appendicitis in
with companies associated with products or services that children. Pediatr Emerg Care. 2007;23:69-76.
significantly impact the specific aspect of disease addressed 20. van den Broek WT, van der Ende ED, Bijnen AB, et al. Which
in the critical question. children could benefit from additional diagnostic tools in case of
suspected appendicitis? J Pediatr Surg. 2004;39:570-574.
21. Klein MD, Rabbani AB, Rood KD, et al. Three quantitative
REFERENCES approaches to the diagnosis of abdominal pain in children:
1. American College of Emergency Physicians. Clinical policy: critical practical applications of decision theory. J Pediatr Surg. 2001;36:
issues for the initial evaluation and management of patients 1375-1380.
presenting with a chief complaint of nontraumatic acute 22. Jacobs JE, Birnbaum BA, Macari M, et al. Acute appendicitis:
abdominal pain. Ann Emerg Med. 2000;36:406-415. comparisons of helical CT diagnosisfocused technique with oral
2. Centers for Disease Control and Prevention. CDC releases latest contrast material versus nonfocused technique with oral and
data on emergency department visits. Advance Data number 340. intravenous contrast material. Radiology. 2001;220:683-690.
2004-1250. Accessed January 26, 2009. Available at: http:// 23. Tamburrini S, Brunetti A, Brown M, et al. Acute appendicitis:
www.cdc.gov/nchs/pressroom/04facts/emergencydept.htm. diagnostic value of nonenhanced CT with selective use of
3. Kachalia A, Gandhi TK, Puopolo AL, et al. Missed and delayed contrast in routine clinical settings. Eur Radiol. 2007;17:2055-
diagnoses in the emergency department: a study of closed 2061.
malpractice claims from 4 liability insurers. Ann Emerg Med. 24. Funaki B, Grosskreutz SR, Funake CN. Using unenhanced helical
2007;49:196-205. CT with enteric contrast material for suspected appendicitis in
4. Selbst SM, Friedman MJ, Singh SB: Epidemiology and etiology of patients treated at a community hospital. AJR Am J Roentgenol.
malpractice lawsuits involving children in US emergency 1998;171:997-1001.
departments and urgent care centers. Pediatr Emerg Care. 2005; 25. Giuliano V, Giuliano C, Pinto F, et al. CT method for visualization
21:165-169. of the appendix using a fixed oral dosage of diatrizoate clinical
5. Bundy DG, Byerley JS, Liles EA, et al. Does this child have experience in 525 cases. Emerg Radiol. 2005;11:281-285.
appendicitis? JAMA. 2007;298:438-451. 26. Ege G, Akman H, Sahin A, et al. Diagnostic value of unenhanced
6. Schriger DL, Cantrill SV, Greene CS. The origins, benefits, harms, helical CT in adult patients with suspected acute appendicitis.
and implications of emergency medicine clinical policies. Ann Br J Radiol. 2002;75:721-725.
Emerg Med. 1993;22:597-602. 27. Lane MJ, Katz DS, Ross BA, et al. Unenhanced helical CT for
7. Wagner JM, McKinney WP, Carpenter JL. Does this patient have suspected acute appendicitis. AJR Am J Roentgenol. 1997;168:
appendicitis? JAMA. 1996;276:1589-1594. 405-409.
8. Andersson REB. Meta-analysis of the clinical and laboratory 28. Wijetunga R, Tan BS, Rouse JC, et al. Diagnostic accuracy of
diagnosis of appendicitis. Br J Surg. 2004;91:28-37. focused appendiceal CT in clinically equivocal cases of acute
9. Gwynn LK. The diagnosis of acute appendicitis: clinical appendicitis. Radiology. 2001;221:747-753.
assessment versus computed tomography evaluation. J Emerg 29. Raman SS, Lu DSK, Kadell BM, et al. Accuracy of nonfocused
Med. 2001;21:119-123. helical CT for the diagnosis of acute appendicitis: a 5-year review.
10. Tzanakis NE, Efstathiou SP, Danulidis K, et al. A new approach to AJR Am J Roentgenol. 2002;178:1319-1325.
accurate diagnosis of acute appendicitis. World J Surg. 2005;29: 30. Ujiki MB, Murayama KM, Cribbins AJ, et al. CT scan in the
1151-1156. management of acute appendicitis. J Surg Res. 2002;105:119-
11. Cardall T, Glasser J, Guss DA. Clinical value of the total white 122.
blood cell count and temperature in the evaluation of patients 31. Malone AJ Jr, Wolf CR, Malmed AS, et al. Diagnosis of acute
with suspected appendicitis. Acad Emerg Med. 2004;11:1021- appendicitis: value of unenhanced CT. AJR Am J Roentgenol.
1027. 1993;160:763-766.
12. Kessler N, Cyteval C, Gallix B, et al. Appendicitis: evaluation of 32. Hershko DD, Awad N, Fischer D, et al. Focused helical CT using
sensitivity, specificity, and predictive values of US, Doppler US, rectal contrast material only as the preferred technique for the
and laboratory findings. Radiology. 2004;230:472-478. diagnosis of suspected acute appendicitis: a prospective,
13. Birchley D. Patients with clinical acute appendicitis should have randomized, controlled study comparing three different
pre-operative full blood count and C-reactive protein assays. Ann techniques. Dis Colon Rectum. 2007;50:1223-1229.
R Coll Surg Engl. 2006;88:27-32. 33. int Hof KH, van Lankeren W, Krestin GP, et al. Surgical validation
14. Alvarado A. A practical score for the early diagnosis of acute of unenhanced helical computed tomography in acute
appendicitis. Ann Emerg Med. 1986;15:557-564. appendicitis. Br J Surg. 2004;91:1641-1645.
15. McKay R, Shepherd J. The use of the clinical scoring system by 34. Lane MJ, Liu DM, Huynh MD, et al. Suspected acute appendicitis:
Alvarado in the decision to perform computed tomography for nonenhanced helical CT in 300 consecutive patients. Radiology.
acute appendicitis in the ED. Am J Emerg Med. 2007;25:489- 1999;213:341-346.
493. 35. Cakirer S, Basak M, Colakoglu B, et al. Diagnosis of acute
16. Chan MYP, Tan C, Chiu MT, et al. Alvarado score: an admission appendicitis with unenhanced helical CT: a study of 130 patients.
criterion in patients with right iliac fossa pain. Surg J R Coll Surg Emerg Radiol. 2002;9:155-161.
Edinb Irel. 2003;1:39-41. 36. Horton MD, Counter SF, Florence MG, et al. A prospective trial of
17. Yildirim E, Karagulle E, Kirbas I, et al. Alvarado scores and pain computed tomography and ultrasonography for diagnosing
onset in relation to multislice CT findings in acute appendicitis. appendicitis in the atypical patient. Am J Surg. 2000;179:379-
Diagn Interv Radiol. 2008;14:14-18. 381.
80 Annals of Emergency Medicine Volume , . : January
Clinical Policy
37. Balthazar EJ, Megibow AJ, Siegel SE, et al. Appendicitis: 55. Baldisserotto M, Marchiori E. Accuracy of noncompressive
prospective evaluation with high-resolution CT. Radiology. 1991; sonography of children with appendicitis according to the
180:21-24. potential positions of the appendix. AJR Am J Roentgenol. 2000;
38. Hershko DD, Sroka G, Bahouth H, et al. The role of selective 175:1387-1392.
computed tomography in the diagnosis and management of 56. Kaiser S, Frenckner B, Jorulf HK. Suspected appendicitis in
suspected acute appendicitis. Am Surg. 2002;68:1003-1007. children: US and CTa prospective randomized study. Radiology.
39. Kamel IR, Goldberg SN, Keogan MT, et al. Right lower quadrant 2002;223:633-638.
pain and suspected appendicitis: nonfocused appendiceal CT 57. Chang CC, Tsai CY, Lin CC, et al. Comparison between
review of 100 cases. Radiology. 2000;217:159-163. technetium-99m hexamethylpropyleneamineoxide labeled white
40. Schuler JG, Shortsleeve MJ, Goldenson RS, et al. Is there a role blood cell abdomen scan and abdominal sonography to detect
for abdominal computed tomographic scans in appendicitis? Arch appendicitis in children with an atypical clinical presentation.
Surg. 1998;133:373-377.
Hepatogastroenterology. 2003;50:426-429.
41. Rao PM, Rhea JT, Novelline RA, et al. Helical CT combined with
58. Dilley A, Wesson D, Munden M, et al. The impact of ultrasound
contrast material administered only through the colon for imaging
examinations on the management of children with suspected
of suspected appendicitis. AJR Am J Roentgenol. 1997;169:
appendicitis: a 3-year analysis. J Pediatr Surg. 2001;36:303-308.
1275-1280.
59. Lowe LH, Penney MW, Stein SM, et al. Unenhanced limited CT of
42. Pickuth D, Spielmann RP. Unenhanced spiral CT for evaluating
acute appendicitis in daily routine. A prospective study. the abdomen in the diagnosis of appendicitis in children:
Hepatogastroenterology. 2001;48:140-142. comparison with sonography. AJR Am J Roentgenol. 2001;176:
43. Walker S, Haun W, Clark J, et al. The value of limited computed 31-35.
tomography with rectal contrast in the diagnosis of acute 60. Sivit CJ, Applegate KE, Stallion A, et al. Imaging evaluation of
appendicitis. Am J Surg. 2000;180:450-455. suspected appendicitis in a pediatric population: effectiveness of
44. Wong SK, Chan LP, Yeo A. Helical CT imaging of clinically sonography versus CT. AJR Am J Roentgenol. 2000;175:977-980.
suspected appendicitis: correlation of CT and histological 61. Teo EL, Tan KP, Lam SL, et al. Ultrasonography and computed
findings. Clin Radiol. 2002;57:741-745. tomography in a clinical algorithm for the evaluation of suspected
45. DIppolito G, Netto de Mello GG, Szejnfeld J. The value of acute appendicitis in children. Singapore Med J. 2000;41:387-
unenhanced CT in the diagnosis of acute appendicitis. Sao Paulo 392.
Med J. 1998;116:1838-1845. 62. Kaiser S, Finnbogason T, Jorulf HK, et al. Suspected appendicitis
46. Morris KT, Kavanagh M, Hansen P, et al. The rational use of in children: diagnosis with contrast-enhanced versus
computed tomography scans in the diagnosis of appendicitis. nonenhanced helical CT. Radiology. 2004;231:427-433.
Am J Surg. 2002;183:547-550. 63. Acosta R, Crain EF, Goldman HS. CT can reduce hospitalization
47. Naffaa LN, Ishak GE, Haddad MC. The value of contrast-enhanced for observation in children with suspected appendicitis. Pediatr
helical CT scan with rectal contrast enema in the diagnosis of Radiol. 2005;35:495-500.
acute appendicitis. J Clin Imaging. 2005;29:255-258. 64. Hoecker CC, Billman GF. The utility of unenhanced computed
48. Rao PM, Rhea JT, Novelline RA, et al. Helical CT technique for the tomography in appendicitis in children. J Emerg Med. 2005;28:
diagnosis of appendicitis: prospective evaluation of a focused 415-421.
appendix CT examination. Radiology. 1997;202:139-144. 65. Mullins ME, Kircher MF, Ryan DP, et al. Evaluation of suspected
49. Mun S, Ernst RD, Chen K, et al. Rapid CT diagnosis of acute appendicitis in children using limited helical CT and colonic
appendicitis with IV contrast material. Emerg Radiol. 2006;12:99- contrast material. AJR Am J Roentgenol. 2001;176:37-41.
102.
66. Kharbanda AB, Taylor GA, Bachur RG. Suspected appendicitis in
50. Anderson BA, Salem L, Flum DR. A systematic review of whether
children: rectal and intravenous contrast-enhanced versus
oral contrast is necessary for the computed tomography
intravenous contrast-enhanced CT. Radiology. 2007;243:520-
diagnosis of appendicitis in adults. Am J Surg. 2005;190:474-
526.
478.
67. Brody AS, Frush DP, Huda W, et al. Radiation risk to children
51. Mittal VK, Goliath J, Sabir M, et al. Advantages of focused helical
computed tomographic scanning with rectal contrast only vs triple from computed tomography. Pediatrics. 2007;120:677-682.
contrast in the diagnosis of clinically uncertain acute 68. American Academy of Pediatrics. Committee on Environmental
appendicitis. A prospective randomized study. Arch Surg. 2004; Health. Risk of ionizing radiation exposure to children: a subject
139:495-500. review. Pediatrics. 1998;101:717-719.
52. Bendeck SE, Nino-Murcia M, Berry GJ, et al. Imaging for 69. Brenner DJ, Hall EJ. Computed tomographyan increasing source
suspected appendicitis: negative appendectomy and perforation of radiation exposure. N Engl J Med. 2007;357:2277-2284.
rates. Radiology. 2002;225:131-136. 70. Garcia Pena BM, Taylor GA, Fishman SJ, et al. Effect of an
53. Yao CC, Lin CS, Yang CC. Laparoscopic appendectomy for imaging protocol on clinical outcomes among pediatric patients
ruptured appendicitis. Surg Laparosc Endosc Percutan Tech. with appendicitis. Pediatrics. 2002;110:1088-1093.
1999;9:271-273. 71. Wan MJ, Krahn M, Ungar WJ, et al. Acute appendicitis in young
54. Klempa I. Current therapy of complicated appendicitis. Chirurg. children: cost-effectiveness of US versus CT in diagnosisa
2002;73:799-804. Markov decision analytic model. Radiology. 2009;250:378-386.
Volume , . : January Annals of Emergency Medicine 81
Clinical Policy
82 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 83
Clinical Policy
84 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 85
Clinical Policy
86 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 87
Clinical Policy
88 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 89
Clinical Policy
90 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 91
Clinical Policy
92 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 93
Clinical Policy
94 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 95
Clinical Policy
96 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 97
Clinical Policy
98 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 99
Clinical Policy
100 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 101
Clinical Policy
102 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 103
Clinical Policy
104 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 105
Clinical Policy
106 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 107
Clinical Policy
108 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 109
Clinical Policy
110 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 111
Clinical Policy
112 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 113
Clinical Policy
114 Annals of Emergency Medicine Volume , . : January
Clinical Policy
Volume , . : January Annals of Emergency Medicine 115
Clinical Policy
Appendix A. Literature classification schema.*
Design/Class Therapy Diagnosis Prognosis
1 Randomized, controlled trial or meta-analyses Prospective cohort using a Population prospective cohort
of randomized trials criterion standard
2 Nonrandomized trial Retrospective observational Retrospective cohort
Case control
3 Case series Case series Case series
Case report Case report Case report
Other (eg, consensus, review) Other (eg, consensus, review) Other (eg, consensus, review)
*Some designs (eg, surveys) will not fit this schema and should be assessed individually.
Objective is to measure therapeutic efficacy comparing 2 interventions.
Objective is to determine the sensitivity and specificity of diagnostic tests.
Objective is to predict outcome including mortality and morbidity.
Appendix B. Approach to downgrading strength of evidence Appendix C. Likelihood ratios.
Design/Class LR () LR (-)
Downgrading 1 2 3 1.0 1.0 Useless
1-5 0.5-1 Rarely of value, only minimally changes pretest
None I II III
probability
1 level II III X
10 0.1 Worthwhile test, may be diagnostic if the result
2 levels III X X
is concordant with pretest probability
Fatally flawed X X X
20 0.05 Strong test, usually diagnostic
100 0.01 Very accurate test, almost always diagnostic
even in the setting of low pretest probability
116 Annals of Emergency Medicine Volume , . : January
Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Early Pregnancy 2012Documento38 pagineEarly Pregnancy 2012Jack GardnerNessuna valutazione finora
- Ahfs2007 PDFDocumento43 pagineAhfs2007 PDFJack GardnerNessuna valutazione finora
- Child Less Than 3 FeverDocumento16 pagineChild Less Than 3 FeverJack GardnerNessuna valutazione finora
- Critical Issues in The Diagnosis and Management of The Adult Psychiatric Patient in The Emergency DepartmentDocumento21 pagineCritical Issues in The Diagnosis and Management of The Adult Psychiatric Patient in The Emergency DepartmentJack GardnerNessuna valutazione finora
- CP PneumoniaDocumento28 pagineCP PneumoniaJack GardnerNessuna valutazione finora
- Opioids 2012Documento27 pagineOpioids 2012Jack GardnerNessuna valutazione finora
- Fountain Head IMDocumento19 pagineFountain Head IMJack GardnerNessuna valutazione finora
- Syncope2007 PDFDocumento14 pagineSyncope2007 PDFOdranoelRichamNessuna valutazione finora
- PE Final 2011Documento100 paginePE Final 2011Jack GardnerNessuna valutazione finora
- E LarynxDocumento1 paginaE LarynxJack GardnerNessuna valutazione finora
- MCQ Atls 9TH Ed 1Documento17 pagineMCQ Atls 9TH Ed 1Ahmed Attia90% (145)
- Cheat SheetDocumento2 pagineCheat SheetJack GardnerNessuna valutazione finora
- Cheat SheetDocumento2 pagineCheat SheetJack GardnerNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Ebp (Evidence-Based Practice)Documento11 pagineEbp (Evidence-Based Practice)TrishaNessuna valutazione finora
- PROGNOSIS EbmDocumento25 paginePROGNOSIS EbmcarinasheliaNessuna valutazione finora
- NCM 109 Course Syllabus Ay 2022 2023Documento17 pagineNCM 109 Course Syllabus Ay 2022 2023ShainaChescaEvans100% (1)
- Learning Clinical Reasoning 2nd Edition-KassirerDocumento352 pagineLearning Clinical Reasoning 2nd Edition-KassirerRutvik Shah88% (8)
- Review: Historical Origins of Evidence-Based MedicineDocumento9 pagineReview: Historical Origins of Evidence-Based MedicineAna PaulaNessuna valutazione finora
- Evidence Based DesignDocumento4 pagineEvidence Based Designmartinadam82Nessuna valutazione finora
- Comorbidity GuidelinesDocumento231 pagineComorbidity Guidelinesgavinbuzz100% (1)
- Empirically Supported Complexity: Rethinking Evidence-Based Practice in PsychotherapyDocumento6 pagineEmpirically Supported Complexity: Rethinking Evidence-Based Practice in PsychotherapyPedro VargasNessuna valutazione finora
- Evidence-Based Medicine and Hospital Reform - Tracing Origins Back To Florence Nightingale - PMC 2Documento10 pagineEvidence-Based Medicine and Hospital Reform - Tracing Origins Back To Florence Nightingale - PMC 2oluwasegunNessuna valutazione finora
- Nursing Process Worksheet SAMPLE 2Documento3 pagineNursing Process Worksheet SAMPLE 2Jaya ReyesNessuna valutazione finora
- Competences Required For Effective Systemic TherapiesDocumento27 pagineCompetences Required For Effective Systemic TherapiesJosé BernalNessuna valutazione finora
- Neck Pain Revision 2017Documento83 pagineNeck Pain Revision 2017Iana VieiraNessuna valutazione finora
- 2017 JN - MC A-New-Therapy PDFDocumento54 pagine2017 JN - MC A-New-Therapy PDFRaudreyNessuna valutazione finora
- Bronquiolite Guidelines AAPDocumento32 pagineBronquiolite Guidelines AAPDiego Guedes da SilvaNessuna valutazione finora
- MC3 - Microbiology and ParasitologyDocumento12 pagineMC3 - Microbiology and ParasitologyChelleyOllitro75% (4)
- Ju: Cebs: Higher Diploma Programme For Teacher EducatorsDocumento232 pagineJu: Cebs: Higher Diploma Programme For Teacher Educatorsmubarek oumerNessuna valutazione finora
- A Comparison of Guidelines For The Treatment of SchizophreniaDocumento3 pagineA Comparison of Guidelines For The Treatment of Schizophreniamonkey85222Nessuna valutazione finora
- Div. Memo 30 S. 2023. Adoption of The Research Management Guidelines in SDO MasbateDocumento59 pagineDiv. Memo 30 S. 2023. Adoption of The Research Management Guidelines in SDO MasbateJuvelyn CabatañaNessuna valutazione finora
- Business Policy Process, Analysis and Coporate GovernanceDocumento4 pagineBusiness Policy Process, Analysis and Coporate GovernanceCOT Management Training InsituteNessuna valutazione finora
- Diagnosis of Acute Gout: A Clinical Practice Guideline From The American College of PhysiciansDocumento8 pagineDiagnosis of Acute Gout: A Clinical Practice Guideline From The American College of PhysiciansRgm UyNessuna valutazione finora
- Ebm Wardwork Orientation: Madeleine Grace M. Sosa, MD Chair, Dept. of Clinical EpidemiologyDocumento73 pagineEbm Wardwork Orientation: Madeleine Grace M. Sosa, MD Chair, Dept. of Clinical EpidemiologyMonica ArmonioNessuna valutazione finora
- Lesson PlansDocumento626 pagineLesson PlansAngie Montala Reana100% (2)
- Human Behavior in Organizations PDF WholeDocumento121 pagineHuman Behavior in Organizations PDF Wholewords of Ace.Nessuna valutazione finora
- Clinical Epidemiology - The Essentials (PDFDrive)Documento349 pagineClinical Epidemiology - The Essentials (PDFDrive)Mirna WidasriNessuna valutazione finora
- Cumulative Course PaperDocumento17 pagineCumulative Course Paperapi-384635531Nessuna valutazione finora
- Hsern Ern's UCS Exam Revision NotesDocumento10 pagineHsern Ern's UCS Exam Revision NotesNanthida AngNessuna valutazione finora
- How Is A Middle Range Nursing Theory Applicable To Your PracticeDocumento7 pagineHow Is A Middle Range Nursing Theory Applicable To Your PracticeSheila KorirNessuna valutazione finora
- Classification of Evidence LevelsDocumento17 pagineClassification of Evidence LevelsDaniela AlejandraNessuna valutazione finora
- MCQ PDFDocumento2 pagineMCQ PDFZainab Al-AliNessuna valutazione finora
- Individual Performance Profile RN Pharmacology Online Practice 2019 ADocumento6 pagineIndividual Performance Profile RN Pharmacology Online Practice 2019 ACaleb LeGearNessuna valutazione finora