Potrebbero piacerti anche
- Podj 3 PDFDocumento2 paginePodj 3 PDFwennyNessuna valutazione finora
- Geographic TongueDocumento2 pagineGeographic TonguewennyNessuna valutazione finora
- Produce101s2 PDFDocumento22 pagineProduce101s2 PDFwennyNessuna valutazione finora
- Oral Pathology - Clinical Pathologic Correlations - 6th - EdDocumento4 pagineOral Pathology - Clinical Pathologic Correlations - 6th - EdwennyNessuna valutazione finora
- GypsumDocumento14 pagineGypsummuskanNessuna valutazione finora
- Textbook of Oral Medicine PDFDocumento1.179 pagineTextbook of Oral Medicine PDFwenny100% (1)
- Sist. Urine 2015 2Documento37 pagineSist. Urine 2015 2wennyNessuna valutazione finora
- AG C O L: Uide To Ommon RAL EsionsDocumento46 pagineAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNessuna valutazione finora
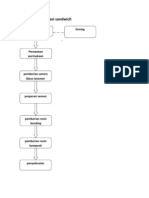
- Teknik dan bahan restorasi sandwichDocumento6 pagineTeknik dan bahan restorasi sandwichMaria Apriliana100% (1)
- AG C O L: Uide To Ommon RAL EsionsDocumento46 pagineAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNessuna valutazione finora
- Handbook of Oral Diseases 1 Edition PDFDocumento30 pagineHandbook of Oral Diseases 1 Edition PDFwennyNessuna valutazione finora
- Geographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewDocumento12 pagineGeographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewwennyNessuna valutazione finora
- 4Documento5 pagine4wennyNessuna valutazione finora
- GypsumDocumento14 pagineGypsummuskanNessuna valutazione finora
- 4Documento5 pagine4wennyNessuna valutazione finora
- Geographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewDocumento12 pagineGeographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewwennyNessuna valutazione finora
- AG C O L: Uide To Ommon RAL EsionsDocumento46 pagineAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNessuna valutazione finora
- Geographic Tongue: Clinical Characteristics of 188 CasesDocumento11 pagineGeographic Tongue: Clinical Characteristics of 188 CaseswennyNessuna valutazione finora
- Dental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteratureDocumento6 pagineDental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteraturewennyNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Patho-Mechanics of Low Back PainDocumento32 pagineThe Patho-Mechanics of Low Back PainydpNessuna valutazione finora
- Prevention of AccidentsDocumento18 paginePrevention of Accidentsapi-27208405Nessuna valutazione finora
- The Painful Shoulder - Part I. Clinical Evaluation. - American Family PhysicianDocumento16 pagineThe Painful Shoulder - Part I. Clinical Evaluation. - American Family PhysicianAdalberto GomesNessuna valutazione finora
- RN - Er Application PacketDocumento56 pagineRN - Er Application PacketJohnny Gto0% (1)
- Referred PainDocumento18 pagineReferred Painapi-3710331Nessuna valutazione finora
- 11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17Documento13 pagine11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17M100% (1)
- Biomechanics of Baseball Pitching: Implications For Injury and Performance Glenn Fleisig American Sports Medicine Institute, Birmingham, AL, USADocumento5 pagineBiomechanics of Baseball Pitching: Implications For Injury and Performance Glenn Fleisig American Sports Medicine Institute, Birmingham, AL, USAYoh ChenNessuna valutazione finora
- stgs6100 stgt6100 t1 TWDocumento20 paginestgs6100 stgt6100 t1 TWjamesfletcherNessuna valutazione finora
- Bone Grafts and SubstitutesDocumento85 pagineBone Grafts and Substitutessandeepvella100% (1)
- Rchimedes Rinciple: by Josep Maria Miró I Coromina Translated by Dustin LanganDocumento54 pagineRchimedes Rinciple: by Josep Maria Miró I Coromina Translated by Dustin LanganMariana CamarasanNessuna valutazione finora
- Clinical Examination of The ShoulderDocumento78 pagineClinical Examination of The ShoulderAbcabc34 AbaNessuna valutazione finora
- Contusion Pulmonum: Clinical Features and ManagementDocumento10 pagineContusion Pulmonum: Clinical Features and ManagementSyamsuriWahyuNessuna valutazione finora
- Hulk Hogan LawsuitDocumento19 pagineHulk Hogan LawsuitLegalBlitz100% (1)
- Mandible Anatomy GuideDocumento96 pagineMandible Anatomy Guidenandani kumariNessuna valutazione finora
- Tube Thoracostomy Chest Tube Implantation and Follow Up: Review ArticleDocumento10 pagineTube Thoracostomy Chest Tube Implantation and Follow Up: Review ArticleAnasthasia hutagalungNessuna valutazione finora
- Minolta Riva Zoom 140Documento80 pagineMinolta Riva Zoom 140Vasile DoroltiNessuna valutazione finora
- Vertical Jump Training ProgramDocumento1 paginaVertical Jump Training Programnicholas_ngo_2Nessuna valutazione finora
- Inguinal Region AnatomyDocumento6 pagineInguinal Region AnatomysimonaNessuna valutazione finora
- HIRA Fabrication WorkshopDocumento316 pagineHIRA Fabrication WorkshopChethan100% (1)
- State of Maharashtra and Ors. Vs Kanchanmala Vijaysing Shirke and ... On 22 August, 1995Documento6 pagineState of Maharashtra and Ors. Vs Kanchanmala Vijaysing Shirke and ... On 22 August, 1995Anonymous KRQaT2PnYqNessuna valutazione finora
- Instruction-Manual CZ 805 BREN enDocumento25 pagineInstruction-Manual CZ 805 BREN enRazza Willi60% (5)
- Handbook of Small Animal Radiological Differential DiagnosisDocumento260 pagineHandbook of Small Animal Radiological Differential DiagnosisLucia CorlatNessuna valutazione finora
- Solar 300 LC - V Operation and Maintenance ManualDocumento244 pagineSolar 300 LC - V Operation and Maintenance ManualEmmanuel solomonNessuna valutazione finora
- 10 Benefits of MarigoldDocumento3 pagine10 Benefits of MarigoldPriya DharshiniNessuna valutazione finora
- MODULE-2-VETTECH325 (2)Documento31 pagineMODULE-2-VETTECH325 (2)cejproiloNessuna valutazione finora
- Posterior Tibialis Tendonitis StudyDocumento6 paginePosterior Tibialis Tendonitis StudyShane WetzelNessuna valutazione finora
- Predicting The Outcome of Perforation Peritonitis by Using Apache II Scoring SystemDocumento5 paginePredicting The Outcome of Perforation Peritonitis by Using Apache II Scoring SystemFarizka Dwinda HNessuna valutazione finora
- ABC TraumaDocumento27 pagineABC TraumarikarzNessuna valutazione finora
- 5 - Mechanical Injury summary-WPS OfficeDocumento28 pagine5 - Mechanical Injury summary-WPS OfficeYazeed AlKhateebNessuna valutazione finora
- DAMS CBT 15 Oct 2017 1Documento121 pagineDAMS CBT 15 Oct 2017 1ReekBhattacharya100% (1)