Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Ob 1.05 Clinical Practice Guidelines On Immunization For Filipino WomenDocumento7 pagineOb 1.05 Clinical Practice Guidelines On Immunization For Filipino Womenotartil_niman50% (2)
- Neurofibromatosis in PregnancyDocumento2 pagineNeurofibromatosis in PregnancyDwi Wahyu AprianiNessuna valutazione finora
- NCP DrainageDocumento3 pagineNCP DrainageRuby GuarinNessuna valutazione finora
- Performance of First Trimester Fetal Ultrasound ScanDocumento12 paginePerformance of First Trimester Fetal Ultrasound ScanPujianti LestarinaNessuna valutazione finora
- Multiple-Choice Questions: Paper 2: A B C D eDocumento35 pagineMultiple-Choice Questions: Paper 2: A B C D eCher'ieie'sa RifirandaNessuna valutazione finora
- Orthopedic Hospital PlanningDocumento7 pagineOrthopedic Hospital Planningሀይደር ዶ.ርNessuna valutazione finora
- NABH 5 STD April 2020Documento120 pagineNABH 5 STD April 2020kapil100% (7)
- Guidelines Ovarian CancerDocumento78 pagineGuidelines Ovarian CancerCher'ieie'sa RifirandaNessuna valutazione finora
- Hyperemesis GravidarumDocumento7 pagineHyperemesis GravidarumPrawira Weka AkbariNessuna valutazione finora
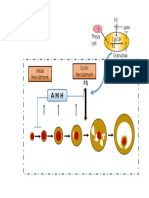
- T Cyp19 A1 T Theca Cell FS H AMHDocumento1 paginaT Cyp19 A1 T Theca Cell FS H AMHCher'ieie'sa RifirandaNessuna valutazione finora
- Role of Oocyte Morphology On Fertilization and Embryo Formation in Assisted Reproductive Techniques.Documento6 pagineRole of Oocyte Morphology On Fertilization and Embryo Formation in Assisted Reproductive Techniques.Cher'ieie'sa RifirandaNessuna valutazione finora
- Syndrome of Newborn: Versus: THE Respiratory Distress THE Immaturity PrematurityDocumento5 pagineSyndrome of Newborn: Versus: THE Respiratory Distress THE Immaturity PrematurityCher'ieie'sa RifirandaNessuna valutazione finora
- 19 Pengukuran Dalam PenelitianDocumento7 pagine19 Pengukuran Dalam PenelitianCher'ieie'sa RifirandaNessuna valutazione finora
- Rymer CHPT 01-29a40fc0rdzDocumento29 pagineRymer CHPT 01-29a40fc0rdzCher'ieie'sa RifirandaNessuna valutazione finora
- An Care Tutor 20 DecDocumento75 pagineAn Care Tutor 20 DecCher'ieie'sa RifirandaNessuna valutazione finora
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Topical Treatment Influencing Systemic ResponseDocumento8 pagineStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Topical Treatment Influencing Systemic ResponseCher'ieie'sa RifirandaNessuna valutazione finora
- Foot UlcersDocumento29 pagineFoot UlcersCher'ieie'sa RifirandaNessuna valutazione finora
- OSCE GuideDocumento184 pagineOSCE GuideKesavaa VasuthavenNessuna valutazione finora
- EoE Clinical Presentation and Co-Morbid ConditionsDocumento20 pagineEoE Clinical Presentation and Co-Morbid ConditionsJulio CesarNessuna valutazione finora
- Assignment On Demography....Documento4 pagineAssignment On Demography....biswasjoyNessuna valutazione finora
- Crash Cart Comp. 2018Documento1 paginaCrash Cart Comp. 2018Roxenette Gil Pangilinan RNNessuna valutazione finora
- Knee Joint Aspiration and InjectionDocumento4 pagineKnee Joint Aspiration and InjectionaimanshalpyNessuna valutazione finora
- Pattern of Neurologic Emergencies in Tikur Anbessa Specialized Hospitalemergency Department in Addis Ababa EthiopiaDocumento5 paginePattern of Neurologic Emergencies in Tikur Anbessa Specialized Hospitalemergency Department in Addis Ababa EthiopiaHelen NeguseNessuna valutazione finora
- NCP Cva Ineffective Tissue PerfusionDocumento1 paginaNCP Cva Ineffective Tissue PerfusionNina Glaiza Goto100% (1)
- ENDOCHAT 162 Uriel JOE 2016 PDFDocumento9 pagineENDOCHAT 162 Uriel JOE 2016 PDFMaria Camila Sarmiento100% (1)
- Effectiveness of Communication Board On Level of Satisfaction Over Communication Among Mechanically Venitlated PatientsDocumento6 pagineEffectiveness of Communication Board On Level of Satisfaction Over Communication Among Mechanically Venitlated PatientsInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Continuing Nursing Education: Importance of Lifelong LearningDocumento6 pagineContinuing Nursing Education: Importance of Lifelong LearningDebashrita MisraNessuna valutazione finora
- Medical and Dental Clearance.1 2017Documento2 pagineMedical and Dental Clearance.1 2017cristina tamonteNessuna valutazione finora
- Dry Eye Syndrome Keratoconjunctivitis SiccaDocumento4 pagineDry Eye Syndrome Keratoconjunctivitis Siccaklinik mandiriNessuna valutazione finora
- Tarsal Tunnel SyndromeDocumento2 pagineTarsal Tunnel SyndromeMuhammad Amri KautsarNessuna valutazione finora
- How Rare Is Heterochromia Iridis?Documento19 pagineHow Rare Is Heterochromia Iridis?Bentoys Street100% (1)
- BBBFDocumento3 pagineBBBFSkAliHassanNessuna valutazione finora
- Maintaining Ethical and Socially Responsible StandardsDocumento1 paginaMaintaining Ethical and Socially Responsible StandardsZarith SofeaNessuna valutazione finora
- S. No. City Name Full Address With Contact No.: List of Our ProductsDocumento3 pagineS. No. City Name Full Address With Contact No.: List of Our Productsprakashrat1962Nessuna valutazione finora
- Position Paper For MUNDocumento2 paginePosition Paper For MUNFarah MustafaNessuna valutazione finora
- Student Response Sheet: PurposeDocumento4 pagineStudent Response Sheet: PurposeYoshi NNessuna valutazione finora
- Unit Plan 3rd Yr 23-24Documento36 pagineUnit Plan 3rd Yr 23-24archana awasthiNessuna valutazione finora
- Role of Ayurveda in Treating Cervical ErosionDocumento9 pagineRole of Ayurveda in Treating Cervical Erosionrazvan rotaruNessuna valutazione finora
- AO CMFS During COVID-19Documento6 pagineAO CMFS During COVID-19โสภาพรรณวดี รวีวารNessuna valutazione finora
- Gambian DHS 2019-20Documento4 pagineGambian DHS 2019-20josetelhadoNessuna valutazione finora
- Incidence of Periventricular/intraventricular Hemorrhage in Very Low Birth Weight Infants: A 15-Year Cohort StudyDocumento7 pagineIncidence of Periventricular/intraventricular Hemorrhage in Very Low Birth Weight Infants: A 15-Year Cohort StudyGusBlomkvistSomocurioNessuna valutazione finora
- Asclepius Consulting IntroductionDocumento3 pagineAsclepius Consulting Introductionapi-3710510Nessuna valutazione finora