Potrebbero piacerti anche
- PH Changes in Radicular Dentine Associated With Calcium Hydroxide and Corticosteroid/antibiotic PastesDocumento7 paginePH Changes in Radicular Dentine Associated With Calcium Hydroxide and Corticosteroid/antibiotic PastesCarolina RomeroNessuna valutazione finora
- External Cervical Resorption: A Three-Dimensional ClassificationDocumento9 pagineExternal Cervical Resorption: A Three-Dimensional ClassificationCarolina RomeroNessuna valutazione finora
- Evaluation of Triple Antibiotic Paste Removal by Different Irrigation ProceduresDocumento6 pagineEvaluation of Triple Antibiotic Paste Removal by Different Irrigation ProceduresCarolina RomeroNessuna valutazione finora
- Guided Endodontics: Accuracy of A Novel Method For Guided Access Cavity Preparation and Root Canal LocationDocumento7 pagineGuided Endodontics: Accuracy of A Novel Method For Guided Access Cavity Preparation and Root Canal LocationCarolina RomeroNessuna valutazione finora
- Choquet Et Al-2001-Journal of PeriodontologyDocumento8 pagineChoquet Et Al-2001-Journal of PeriodontologyCarolina RomeroNessuna valutazione finora
- Incidence and Position of The Canal Isthmus. Part 1. Mesiobuccal Root of The Maxillary First MolarDocumento4 pagineIncidence and Position of The Canal Isthmus. Part 1. Mesiobuccal Root of The Maxillary First MolarCarolina RomeroNessuna valutazione finora
- Incidence and Position of The Canal Isthmus. Part 1. Mesiobuccal Root of The Maxillary First MolarDocumento4 pagineIncidence and Position of The Canal Isthmus. Part 1. Mesiobuccal Root of The Maxillary First MolarCarolina RomeroNessuna valutazione finora
- Aneurysmal Bone Cyst of The Mandible: Case Presentation and Review of The LiteratureDocumento3 pagineAneurysmal Bone Cyst of The Mandible: Case Presentation and Review of The LiteratureCarolina RomeroNessuna valutazione finora
- Review: Osseointegration of Dental Implants in Patients Undergoing Bisphosphonate Treatment: A Literature ReviewDocumento6 pagineReview: Osseointegration of Dental Implants in Patients Undergoing Bisphosphonate Treatment: A Literature ReviewCarolina Romero100% (1)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Assessing Inclusive Ed-PhilDocumento18 pagineAssessing Inclusive Ed-PhilElla MaglunobNessuna valutazione finora
- DNV Rules For Electrical Instal at IonsDocumento80 pagineDNV Rules For Electrical Instal at Ionsnzjohn100% (3)
- Corn Pulao Recipe With Sweet CornDocumento2 pagineCorn Pulao Recipe With Sweet CornSudharshanNessuna valutazione finora
- Undas Deployment PadsDocumento15 pagineUndas Deployment PadsVic NairaNessuna valutazione finora
- (9F) Ankle - Bones, Joints, Tendons and LigamentsDocumento4 pagine(9F) Ankle - Bones, Joints, Tendons and LigamentsJeffrey RamosNessuna valutazione finora
- Smart Goals ExerciseDocumento2 pagineSmart Goals Exerciseapi-594661640Nessuna valutazione finora
- Power Systems-III Ditital NotesDocumento102 paginePower Systems-III Ditital NotesSimranNessuna valutazione finora
- English 10 - HVC - ĐềDocumento22 pagineEnglish 10 - HVC - ĐềAlin NguyenNessuna valutazione finora
- The Turbo Air 6000 Centrifugal Compressor Handbook AAEDR-H-082 Rev 05 TA6000Documento137 pagineThe Turbo Air 6000 Centrifugal Compressor Handbook AAEDR-H-082 Rev 05 TA6000Rifki TriAditiya PutraNessuna valutazione finora
- The Congressional Committee and Philippine Policymaking: The Case of The Anti-Rape Law - Myrna LavidesDocumento29 pagineThe Congressional Committee and Philippine Policymaking: The Case of The Anti-Rape Law - Myrna LavidesmarielkuaNessuna valutazione finora
- Abnegation Faction:: Clothing Is Gray and Simple. The OnlyDocumento7 pagineAbnegation Faction:: Clothing Is Gray and Simple. The OnlylethaagathaNessuna valutazione finora
- Reading 1Documento2 pagineReading 1Marcelo BorsiniNessuna valutazione finora
- Otology Fellowships 2019Documento5 pagineOtology Fellowships 2019Sandra SandrinaNessuna valutazione finora
- 2VV-33C-R4-V5 Product SpecificationsDocumento5 pagine2VV-33C-R4-V5 Product Specificationsnhan sieuNessuna valutazione finora
- Rundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967Documento15 pagineRundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967nixyingboNessuna valutazione finora
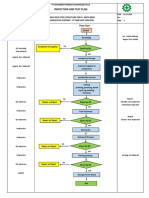
- Inspection and Test Plan: Flow Chart Start IncomingDocumento1 paginaInspection and Test Plan: Flow Chart Start IncomingSinden AyuNessuna valutazione finora
- Edinburgh Postnatal Depression Scale. Detection of Postnatal Depression. Development of The 10-ItemDocumento6 pagineEdinburgh Postnatal Depression Scale. Detection of Postnatal Depression. Development of The 10-ItemKyze LQNessuna valutazione finora
- PE 560 Atomic Absorption Spectrophotometer ManualDocumento176 paginePE 560 Atomic Absorption Spectrophotometer ManualDavid Allan100% (1)
- Lewis Heart Failure Care PlanDocumento4 pagineLewis Heart Failure Care Plansarahbearcoups100% (1)
- SmithfieldDocumento11 pagineSmithfieldandreea143Nessuna valutazione finora
- Thermo Drain 52 Pages - CatalogueDocumento52 pagineThermo Drain 52 Pages - CatalogueSandeep Nair100% (1)
- EMI InstructionsDocumento2 pagineEMI InstructionsAKSHAY ANANDNessuna valutazione finora
- MSE 2103 - Lec 12 (7 Files Merged)Documento118 pagineMSE 2103 - Lec 12 (7 Files Merged)md akibhossainNessuna valutazione finora
- Duty Roster Class IV JulyDocumento2 pagineDuty Roster Class IV JulyTayyab HassanNessuna valutazione finora
- Mri 7 TeslaDocumento12 pagineMri 7 TeslaJEAN FELLIPE BARROSNessuna valutazione finora
- CanteenDocumento8 pagineCanteenmahesh4uNessuna valutazione finora
- Euro 4 Standard PDFDocumento2 pagineEuro 4 Standard PDFCamellaNessuna valutazione finora
- Group 17-Solid State NMR - Questions-AnswersDocumento5 pagineGroup 17-Solid State NMR - Questions-AnswersOmkar AkulwarNessuna valutazione finora
- The Motive Journal (3rd Edition)Documento42 pagineThe Motive Journal (3rd Edition)Shubham Sharma0% (1)
- Carbon Cycle Game Worksheet - EportfolioDocumento2 pagineCarbon Cycle Game Worksheet - Eportfolioapi-264746220Nessuna valutazione finora