Potrebbero piacerti anche
- Pediatric Hematology and Oncology: Scientific Principles and Clinical PracticeDa EverandPediatric Hematology and Oncology: Scientific Principles and Clinical PracticeEdward EstlinNessuna valutazione finora
- LESSON 3 Renal Function and TestsDocumento63 pagineLESSON 3 Renal Function and TestsFaith TambongNessuna valutazione finora
- CH17Documento22 pagineCH17JoshMatthewsNessuna valutazione finora
- Sepsis Neonatal 3Documento13 pagineSepsis Neonatal 3Ega AihenaNessuna valutazione finora
- 2 Tietz 2012 Kidney Function TestsDocumento39 pagine2 Tietz 2012 Kidney Function TestsIvana BajunovicNessuna valutazione finora
- Approach To Chronic Diarrhea in Children - 6 Months in Resource-Rich Countries - UpToDateDocumento15 pagineApproach To Chronic Diarrhea in Children - 6 Months in Resource-Rich Countries - UpToDateNedelcu MirunaNessuna valutazione finora
- Neonatal HypoglycemiaDocumento12 pagineNeonatal HypoglycemiayogaNessuna valutazione finora
- Hypo ToniaDocumento56 pagineHypo ToniaKRITHIKA A/P PALANNY MoeNessuna valutazione finora
- PEDIA - Cardio (Esguerra) PDFDocumento9 paginePEDIA - Cardio (Esguerra) PDFMedisina101Nessuna valutazione finora
- Pediatric Diagnosis PedDocumento153 paginePediatric Diagnosis PedIceNessuna valutazione finora
- EncoperesisDocumento6 pagineEncoperesisRishi SelvamNessuna valutazione finora
- Fiebre Sin Foco 0-36 MesesDocumento28 pagineFiebre Sin Foco 0-36 MesesdanielentuxtlaNessuna valutazione finora
- Important Pediatrics SyndromesDocumento11 pagineImportant Pediatrics SyndromesYogeshRavalNessuna valutazione finora
- Physical Examination of Urine SummaryDocumento3 paginePhysical Examination of Urine SummaryBiancake Sta. AnaNessuna valutazione finora
- GalactosemiaDocumento6 pagineGalactosemiaakbar alituNessuna valutazione finora
- Cerebral Palsy: Prof. V.P.SharmaDocumento34 pagineCerebral Palsy: Prof. V.P.Sharmaخالد القرشيNessuna valutazione finora
- Urine Sediment Particles PDFDocumento119 pagineUrine Sediment Particles PDFambadepravinNessuna valutazione finora
- Corynebacterium and Other Non-spore-Forming Gram-Positive RodsDocumento3 pagineCorynebacterium and Other Non-spore-Forming Gram-Positive RodsYelai CarveroNessuna valutazione finora
- Physiology Review: A Work in ProgressDocumento424 paginePhysiology Review: A Work in ProgressSukhman SeerhaNessuna valutazione finora
- Erythrocytes Related Abnormalities and Diseases: Erythrocytic Morphology and Associated Disease (Size and Shape)Documento5 pagineErythrocytes Related Abnormalities and Diseases: Erythrocytic Morphology and Associated Disease (Size and Shape)rona hilarioNessuna valutazione finora
- Administering Corticosteroids in Neurologic Diseases3724Documento12 pagineAdministering Corticosteroids in Neurologic Diseases3724Carmen BritoNessuna valutazione finora
- Lec 1 - IntroductionDocumento3 pagineLec 1 - IntroductionHaendra Mae DapilagaNessuna valutazione finora
- 06.2 Inborn Error of Metabolism - Iii B - Trans PDFDocumento10 pagine06.2 Inborn Error of Metabolism - Iii B - Trans PDFAshim AbhiNessuna valutazione finora
- Pediatric Intracranial Hypertension: Education GapDocumento11 paginePediatric Intracranial Hypertension: Education GapDiego CedamanosNessuna valutazione finora
- Fresh Tissue ExaminationDocumento6 pagineFresh Tissue ExaminationChiizu iraNessuna valutazione finora
- Part Ii Specimen Collection & Laboratory Diagnosis For VirusesDocumento6 paginePart Ii Specimen Collection & Laboratory Diagnosis For VirusesBONNA FAYE CHRISZEL HUI YING TANNessuna valutazione finora
- Clostrdia: G Positive Spore Forming Anaerobic Toxin Producing RodsDocumento36 pagineClostrdia: G Positive Spore Forming Anaerobic Toxin Producing Rodsjamal nasirNessuna valutazione finora
- VDRL Test and Its InterpretationDocumento11 pagineVDRL Test and Its InterpretationSauZen SalaZarNessuna valutazione finora
- Culturing MicroorganismsDocumento26 pagineCulturing MicroorganismsInsatiable CleeNessuna valutazione finora
- Fever in The Pediatric Patient PDFDocumento24 pagineFever in The Pediatric Patient PDFSABASA1012Nessuna valutazione finora
- Mediators of Inflammation: DR - Djumadi Achmad, Sppa (K)Documento33 pagineMediators of Inflammation: DR - Djumadi Achmad, Sppa (K)Elearning FK UnhasNessuna valutazione finora
- (MT6317) Unit 6.1 Introduction To Carbohydrates and Glucose DeterminationDocumento12 pagine(MT6317) Unit 6.1 Introduction To Carbohydrates and Glucose DeterminationJC DomingoNessuna valutazione finora
- Histopath Lec (Module 1) : Iintroduction To PathologyDocumento17 pagineHistopath Lec (Module 1) : Iintroduction To PathologyAngela ReyesNessuna valutazione finora
- BeyondSurvival 2nd Edition enDocumento86 pagineBeyondSurvival 2nd Edition enJonhie SamayoaNessuna valutazione finora
- FalciparumDocumento4 pagineFalciparumDandun Dannie-DunNessuna valutazione finora
- Histopathologic TechniquesDocumento78 pagineHistopathologic TechniquesSwitzel CustodioNessuna valutazione finora
- SELF STUDY Specimen Collection and TransportDocumento3 pagineSELF STUDY Specimen Collection and TransportAngelic AngelesNessuna valutazione finora
- Purine Disorder PDFDocumento1 paginaPurine Disorder PDFAnya IgnacioNessuna valutazione finora
- Midterm ParasitologyDocumento18 pagineMidterm ParasitologyAngelic AngelesNessuna valutazione finora
- Aub F Urine Screening For Metabolic DisordersDocumento4 pagineAub F Urine Screening For Metabolic DisordersRomie SolacitoNessuna valutazione finora
- Use of C-Reactive Protein and Ferritin Biomarkers in Daily Pediatric PracticeDocumento14 pagineUse of C-Reactive Protein and Ferritin Biomarkers in Daily Pediatric PracticeMichelleHanNessuna valutazione finora
- Iron Kinetics and Laboratory AssessmentDocumento4 pagineIron Kinetics and Laboratory AssessmentJohnree A. EvangelistaNessuna valutazione finora
- Urease Test - Principle, Media, Procedure and ResultDocumento11 pagineUrease Test - Principle, Media, Procedure and ResultAlisha KhanNessuna valutazione finora
- Slide Pediatric TuberculosisDocumento112 pagineSlide Pediatric TuberculosisFenny RahmadaniNessuna valutazione finora
- Parasitology PRKTKLDocumento58 pagineParasitology PRKTKLmohamed100% (2)
- Arachnoid CystDocumento18 pagineArachnoid CystMirunalakshmi M100% (2)
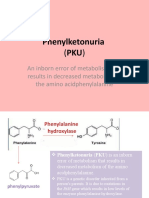
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocumento8 paginePhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNessuna valutazione finora
- Venipuncture Complications and Preexamination Variables: RequistionsDocumento19 pagineVenipuncture Complications and Preexamination Variables: RequistionsAngel Cascayan Delos SantosNessuna valutazione finora
- Coagulation 1Documento12 pagineCoagulation 1kriss WongNessuna valutazione finora
- Microanatomy pt1Documento27 pagineMicroanatomy pt1poopziNessuna valutazione finora
- Parasite Lab 5 Helminths PDF (M)Documento18 pagineParasite Lab 5 Helminths PDF (M)Ali RonaldoNessuna valutazione finora
- Hematology Written SummariesDocumento6 pagineHematology Written SummariesDrexler Ray EukanNessuna valutazione finora
- Medical Parasitology: Medina & Albano - Lecture & LaboratoryDocumento9 pagineMedical Parasitology: Medina & Albano - Lecture & LaboratoryabigailNessuna valutazione finora
- Gram Positive: CoccusDocumento8 pagineGram Positive: CoccusLM MysNessuna valutazione finora
- Structure of Prion: The Normal Prion Structure Is Characterized by Four Helices, Denoted As PRPCDocumento14 pagineStructure of Prion: The Normal Prion Structure Is Characterized by Four Helices, Denoted As PRPCMatthew WilsonNessuna valutazione finora
- Human Papilloma VirusDocumento29 pagineHuman Papilloma Virusphone pyaeNessuna valutazione finora
- Gram Positive CocciDocumento34 pagineGram Positive CocciMaria Cecilia Flores50% (2)
- IMH Laboratory ManualDocumento56 pagineIMH Laboratory ManualHaniya KhanNessuna valutazione finora
- AUBF - Chapter 2Documento5 pagineAUBF - Chapter 2Kristin SoquilloNessuna valutazione finora
- AUBF Lecture Chemical Examination of UrineDocumento6 pagineAUBF Lecture Chemical Examination of UrineJane Yvette AndresNessuna valutazione finora
- Laboratory Management PDFDocumento99 pagineLaboratory Management PDFPam Fajardo100% (5)
- A Timeline of Death Penalty in The PhilippinesDocumento5 pagineA Timeline of Death Penalty in The PhilippinesPam FajardoNessuna valutazione finora
- 11 Constructing A Thesis StatementDocumento3 pagine11 Constructing A Thesis StatementPam FajardoNessuna valutazione finora
- History of Medical TechnologyDocumento19 pagineHistory of Medical TechnologyPam FajardoNessuna valutazione finora
- Which Statistical Tests To UseDocumento1 paginaWhich Statistical Tests To UsePam FajardoNessuna valutazione finora
- Normal DistributionDocumento24 pagineNormal DistributionPam FajardoNessuna valutazione finora
- Lab Safety ImmunoDocumento24 pagineLab Safety ImmunoPam FajardoNessuna valutazione finora
- Which Statistical Tests To UseDocumento1 paginaWhich Statistical Tests To UsePam FajardoNessuna valutazione finora
- 07 Apa Style EssentialsDocumento3 pagine07 Apa Style EssentialsPam FajardoNessuna valutazione finora
- 07 Apa Style EssentialsDocumento3 pagine07 Apa Style EssentialsPam FajardoNessuna valutazione finora
- Laboratory Safety HEMA Chapter 2Documento34 pagineLaboratory Safety HEMA Chapter 2Pam FajardoNessuna valutazione finora
- 01 The Nature of Writing PDFDocumento2 pagine01 The Nature of Writing PDFPam Fajardo88% (8)
- Biostat NotesDocumento8 pagineBiostat NotesPam FajardoNessuna valutazione finora
- Graph X-Axis CM Y-Axis 2 Cums: Blood Glucose (Binned)Documento3 pagineGraph X-Axis CM Y-Axis 2 Cums: Blood Glucose (Binned)Pam FajardoNessuna valutazione finora
- BCSL 058 Previous Year Question Papers by IgnouassignmentguruDocumento45 pagineBCSL 058 Previous Year Question Papers by IgnouassignmentguruSHIKHA JAINNessuna valutazione finora
- Handbook For ASHA On Home Based Care For Young Child-EnglishDocumento116 pagineHandbook For ASHA On Home Based Care For Young Child-EnglishDr. Vanitha BNessuna valutazione finora
- Presentation 1Documento7 paginePresentation 1Abdillah StrhanNessuna valutazione finora
- Qa/Qc Mechanical Monthly Progress Report For June 2015: Area/System Description Status RemarksDocumento1 paginaQa/Qc Mechanical Monthly Progress Report For June 2015: Area/System Description Status RemarksRen SalazarNessuna valutazione finora
- CFD Analysis of Flow Through Compressor CascadeDocumento10 pagineCFD Analysis of Flow Through Compressor CascadeKhalid KhalilNessuna valutazione finora
- Introduction To Kalman FilterDocumento4 pagineIntroduction To Kalman FilterArghya MukherjeeNessuna valutazione finora
- Chemical Process DebottleneckingDocumento46 pagineChemical Process DebottleneckingAhmed Ansari100% (2)
- Accessories 162-USDocumento20 pagineAccessories 162-USعايد التعزيNessuna valutazione finora
- What A Wonderful WorldDocumento3 pagineWhat A Wonderful Worldapi-333684519Nessuna valutazione finora
- Wet Chemical Pre E PresentationDocumento310 pagineWet Chemical Pre E PresentationEdwardAlexanderGarciaNessuna valutazione finora
- Company Profile Pt. KPT PDFDocumento23 pagineCompany Profile Pt. KPT PDFfery buyaNessuna valutazione finora
- Anchor Chart-Describing Words-Descriptive Details of Setting and Character PDFDocumento2 pagineAnchor Chart-Describing Words-Descriptive Details of Setting and Character PDFdellindiaNessuna valutazione finora
- Ora Laboratory Manual: Section 1 Section 1Documento36 pagineOra Laboratory Manual: Section 1 Section 1Ahmed IsmailNessuna valutazione finora
- مشخصات فنی بیل بکهو فیات کوبلکو b200Documento12 pagineمشخصات فنی بیل بکهو فیات کوبلکو b200Maryam0% (1)
- Farmhouse Style Plans - Farm & CountryDocumento6 pagineFarmhouse Style Plans - Farm & Countryhanif azriNessuna valutazione finora
- Chapter 4 Occupational Safety Hazards in Food Service OperationsDocumento14 pagineChapter 4 Occupational Safety Hazards in Food Service OperationsStraichea Mae TabanaoNessuna valutazione finora
- Strange Christmas TraditionsDocumento2 pagineStrange Christmas TraditionsZsofia ZsofiaNessuna valutazione finora
- Motorcycle Troubleshooting ManualDocumento15 pagineMotorcycle Troubleshooting ManualJan Warmerdam100% (1)
- The Latent Phase of LaborDocumento8 pagineThe Latent Phase of LaborLoisana Meztli Figueroa PreciadoNessuna valutazione finora
- Medical CodingDocumento5 pagineMedical CodingBernard Paul GuintoNessuna valutazione finora
- Bomber JacketDocumento3 pagineBomber JacketLaura Carrascosa FusterNessuna valutazione finora
- DEAD STARS by Paz Marquez BenitezDocumento17 pagineDEAD STARS by Paz Marquez BenitezArmiethazen Khea Page PalarcaNessuna valutazione finora
- Aesa Based Pechay Production - AbdulwahidDocumento17 pagineAesa Based Pechay Production - AbdulwahidAnne Xx100% (1)
- HACH LANGE Amino Acid F Reagent Powder (2353255)Documento6 pagineHACH LANGE Amino Acid F Reagent Powder (2353255)kerem__22Nessuna valutazione finora
- Inspirational Quotes General and ExamsDocumento6 pagineInspirational Quotes General and Examsasha jalanNessuna valutazione finora
- Inverse Curve Trip Time Calculation: Enter Values in White CellDocumento3 pagineInverse Curve Trip Time Calculation: Enter Values in White CellVijay FxNessuna valutazione finora
- PositioningDocumento2 paginePositioningKishan AndureNessuna valutazione finora
- 5 160 1 PBDocumento13 pagine5 160 1 PBLotkomoaidone Harahu TukambaNessuna valutazione finora
- No Client Too Far: Flexible Antenna Options TDMA GPS Sync ClientDocumento2 pagineNo Client Too Far: Flexible Antenna Options TDMA GPS Sync ClientFelix MartinezNessuna valutazione finora
- ICH Quality Guidelines: An Implementation GuideDa EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleNessuna valutazione finora
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsDa EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsValutazione: 5 su 5 stelle5/5 (3)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactDa EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactValutazione: 5 su 5 stelle5/5 (5)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincDa EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincValutazione: 3.5 su 5 stelle3.5/5 (137)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideDa EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNessuna valutazione finora
- Chemistry for Breakfast: The Amazing Science of Everyday LifeDa EverandChemistry for Breakfast: The Amazing Science of Everyday LifeValutazione: 4.5 su 5 stelle4.5/5 (14)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactDa EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactValutazione: 5 su 5 stelle5/5 (1)
- It's Elemental: The Hidden Chemistry in EverythingDa EverandIt's Elemental: The Hidden Chemistry in EverythingValutazione: 4 su 5 stelle4/5 (10)
- Chemistry: a QuickStudy Laminated Reference GuideDa EverandChemistry: a QuickStudy Laminated Reference GuideValutazione: 5 su 5 stelle5/5 (1)
- AP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeDa EverandAP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeNessuna valutazione finora
- Guidelines for Defining Process Safety Competency RequirementsDa EverandGuidelines for Defining Process Safety Competency RequirementsValutazione: 3 su 5 stelle3/5 (1)
- AP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeDa EverandAP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeValutazione: 5 su 5 stelle5/5 (1)
- The Production of Volatile Oils and Perfumery Plants in the United StatesDa EverandThe Production of Volatile Oils and Perfumery Plants in the United StatesNessuna valutazione finora
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeDa EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeValutazione: 4 su 5 stelle4/5 (1)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeDa EverandChemistry for Breakfast: The Amazing Science of Everyday LifeValutazione: 4.5 su 5 stelle4.5/5 (90)
- Taste: Surprising Stories and Science About Why Food Tastes GoodDa EverandTaste: Surprising Stories and Science About Why Food Tastes GoodValutazione: 3 su 5 stelle3/5 (20)
- Essential Chemistry for Formulators of Semisolid and Liquid DosagesDa EverandEssential Chemistry for Formulators of Semisolid and Liquid DosagesValutazione: 5 su 5 stelle5/5 (2)