Potrebbero piacerti anche
- Analysis of The Diagnostic Value of CD138 For ChroDocumento8 pagineAnalysis of The Diagnostic Value of CD138 For ChroAntonio RibeiroNessuna valutazione finora
- Medip, IJRCOG-5630 O PDFDocumento5 pagineMedip, IJRCOG-5630 O PDFSuraj NagarajNessuna valutazione finora
- Cervical Cancer Risk Factors in Dr. Soetomo HospitalDocumento6 pagineCervical Cancer Risk Factors in Dr. Soetomo HospitalmonicaNessuna valutazione finora
- Evaluation of Transvaginal Sonography in Detecting Endometrial Polyps and The Pregnancy Outcome Following Hysteroscopic Polypectomy in Infertile WomenDocumento5 pagineEvaluation of Transvaginal Sonography in Detecting Endometrial Polyps and The Pregnancy Outcome Following Hysteroscopic Polypectomy in Infertile WomenMoe AboamNessuna valutazione finora
- Meconium-Stained Amniotic Fluid: A Risk Factor For Postpartum HemorrhageDocumento5 pagineMeconium-Stained Amniotic Fluid: A Risk Factor For Postpartum HemorrhagelaniNessuna valutazione finora
- Hemorrhagic Ovarian CystsDocumento5 pagineHemorrhagic Ovarian CystsPraise ManoppoNessuna valutazione finora
- Ahmadinejad 20Documento8 pagineAhmadinejad 20ayuNessuna valutazione finora
- Hysteroscopy findings in infertilityDocumento38 pagineHysteroscopy findings in infertilityPriyaNessuna valutazione finora
- 6604974a PDFDocumento7 pagine6604974a PDFAbraham Theodore SNessuna valutazione finora
- Yolk Sac Shape OutcomeDocumento11 pagineYolk Sac Shape OutcomeSofyan QadriNessuna valutazione finora
- NIH Public Access: Author ManuscriptDocumento21 pagineNIH Public Access: Author ManuscriptanyNessuna valutazione finora
- Acretismo PlacentarioDocumento9 pagineAcretismo PlacentarioRolando LaraNessuna valutazione finora
- Perbandingan Usg Transvaginal Dan TransabdominalDocumento6 paginePerbandingan Usg Transvaginal Dan TransabdominalrkyaritonangNessuna valutazione finora
- IJHS Robson PublicationDocumento9 pagineIJHS Robson PublicationVinod BharatiNessuna valutazione finora
- Cervical Cancer Risk FactorsDocumento3 pagineCervical Cancer Risk FactorsWindhaNessuna valutazione finora
- 10 1111@jog 143436777777Documento17 pagine10 1111@jog 143436777777Epiphany SonderNessuna valutazione finora
- Systematic Review of Firsttrimester Ultrasound Screening For Detection of Fetal Structural Anomalies and Factors Affecting Screening PerformanceDocumento14 pagineSystematic Review of Firsttrimester Ultrasound Screening For Detection of Fetal Structural Anomalies and Factors Affecting Screening PerformanceMariana B.Nessuna valutazione finora
- CHSJ 48 02 04 2022Documento7 pagineCHSJ 48 02 04 2022mihail.boldeanuNessuna valutazione finora
- SonoDocumento11 pagineSonoghaffari.eli5912Nessuna valutazione finora
- Pregnant Women's Attitudes Toward UltrasoundDocumento6 paginePregnant Women's Attitudes Toward Ultrasoundelda zulkarnainNessuna valutazione finora
- Tratamiento Esofago Cervical Lu, 2021Documento9 pagineTratamiento Esofago Cervical Lu, 2021Carlos N. Rojas PuyolNessuna valutazione finora
- Factores de Riesgo y Resultados de EpisiotomíaDocumento19 pagineFactores de Riesgo y Resultados de EpisiotomíaAlvaro OyarceNessuna valutazione finora
- Cesarean Scar Defect: A Prospective Study On Risk Factors: GynecologyDocumento8 pagineCesarean Scar Defect: A Prospective Study On Risk Factors: Gynecologynuphie_nuphNessuna valutazione finora
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocumento5 pagineEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyGustina Maryanti MooyNessuna valutazione finora
- 19 - Benefits of Cervical Cancer Screening by Liquid-BasedDocumento5 pagine19 - Benefits of Cervical Cancer Screening by Liquid-BasedRenan RodriguesNessuna valutazione finora
- EndometritisDocumento6 pagineEndometritisMuh Syarifullah ANessuna valutazione finora
- Mustafa 2016Documento7 pagineMustafa 2016ejigsonNessuna valutazione finora
- Vaginal Touch Versus Transvaginal Ultrasound in The Management of Threatened Preterm Labour at The University Hospital Center of Porto-Novo (Benin)Documento9 pagineVaginal Touch Versus Transvaginal Ultrasound in The Management of Threatened Preterm Labour at The University Hospital Center of Porto-Novo (Benin)Bayu Diesfa PuteraNessuna valutazione finora
- +xvedqg V 6xsruw WR (Qfrxudjh 3Ds 6phdu 3duwlflsdwlrq Ri) Huwloh &rxsohv LQ 3Xfdqj Gading Residence SemarangDocumento12 pagine+xvedqg V 6xsruw WR (Qfrxudjh 3Ds 6phdu 3duwlflsdwlrq Ri) Huwloh &rxsohv LQ 3Xfdqj Gading Residence SemarangAbynizar Mirojjul FikryNessuna valutazione finora
- Karakteristik Pasien Kanker Serviks Di Rsud Dr. Soetomo Surabaya Periode Januari - Desember 2017Documento4 pagineKarakteristik Pasien Kanker Serviks Di Rsud Dr. Soetomo Surabaya Periode Januari - Desember 2017gita rahayuNessuna valutazione finora
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocumento3 pagineEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyRaissa Metasari TantoNessuna valutazione finora
- Cervical Cancer Screening With Human Papillomavirus DNA and Cytology in JapanDocumento7 pagineCervical Cancer Screening With Human Papillomavirus DNA and Cytology in Japandella kharisma putriNessuna valutazione finora
- Parturition Events and Risk of Urinary Incontinence in Later LifeDocumento16 pagineParturition Events and Risk of Urinary Incontinence in Later LifeMutia LailaniNessuna valutazione finora
- Correlation of Cervical Screening TestsDocumento7 pagineCorrelation of Cervical Screening TestsMarcos HoilNessuna valutazione finora
- Manajemen Plasent AkretaDocumento14 pagineManajemen Plasent AkretaangelNessuna valutazione finora
- Pregnancy Outcomes for Women with First/Second Trimester Subchorionic HemorrhageDocumento7 paginePregnancy Outcomes for Women with First/Second Trimester Subchorionic HemorrhagePalwinder SinghNessuna valutazione finora
- Low-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesDocumento11 pagineLow-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesEduarda QuartinNessuna valutazione finora
- Impact of Oligohydramnios On Maternal and PerinataDocumento6 pagineImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNessuna valutazione finora
- Atm 20 5463Documento9 pagineAtm 20 5463Aline Costales TafoyaNessuna valutazione finora
- MiscarriageDocumento8 pagineMiscarriagejaimejoseNessuna valutazione finora
- Hematoma SubcorionicoDocumento6 pagineHematoma SubcorionicoMagic_OverNessuna valutazione finora
- 2 Erewrf 242Documento5 pagine2 Erewrf 242supaidi97Nessuna valutazione finora
- Role of Ultrasonography in Diagnosis of Ectopic Pregnancy With Clinical Analysis and Management in Tertiary Care HospitalDocumento4 pagineRole of Ultrasonography in Diagnosis of Ectopic Pregnancy With Clinical Analysis and Management in Tertiary Care HospitalRizka AdiNessuna valutazione finora
- Atb of Amniotic Fluid SludgeDocumento20 pagineAtb of Amniotic Fluid SludgeSantiago RollanNessuna valutazione finora
- VBAC Research Evidence and Technique ImplementationDocumento2 pagineVBAC Research Evidence and Technique ImplementationGodfrey AntolinNessuna valutazione finora
- Maternal and Fetal Outcome of Placenta PDocumento5 pagineMaternal and Fetal Outcome of Placenta Pfamelalusu eaNessuna valutazione finora
- Learning Curve in Determining Fetal Sex by First Trimester Ultrasound ScanDocumento6 pagineLearning Curve in Determining Fetal Sex by First Trimester Ultrasound ScanAisahNessuna valutazione finora
- Case 16-2014: A 46-Year-Old Woman in Botswana With Postcoital BleedingDocumento10 pagineCase 16-2014: A 46-Year-Old Woman in Botswana With Postcoital BleedingDesi HutapeaNessuna valutazione finora
- Articol 1Documento7 pagineArticol 1nistor97Nessuna valutazione finora
- Updates in Cervical Cytology: 90 Years of ProgressDocumento11 pagineUpdates in Cervical Cytology: 90 Years of Progressmohamaed abbasNessuna valutazione finora
- Our Experience With Adnexal Masses in The Pediatric Age Group and Review of LiteratureDocumento6 pagineOur Experience With Adnexal Masses in The Pediatric Age Group and Review of LiteratureEdwin CalleNessuna valutazione finora
- Jurnal KPD EnglishDocumento8 pagineJurnal KPD Englishdiah stanyaNessuna valutazione finora
- Caesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort StudyDocumento9 pagineCaesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort Studyluis albenis mendoza guerraNessuna valutazione finora
- 1 s2.0 S1876034119302692 MainDocumento5 pagine1 s2.0 S1876034119302692 MainiffaNessuna valutazione finora
- Jurnal Placenta PreviaDocumento9 pagineJurnal Placenta Previasheva25Nessuna valutazione finora
- Peccatori 2013Documento11 paginePeccatori 2013Alfa KaromahNessuna valutazione finora
- Peccatori2013 PDFDocumento11 paginePeccatori2013 PDFAlfa KaromahNessuna valutazione finora
- Comparison of Transverse and Vertical Skin Incision For Emergency Cesarean DeliveryDocumento7 pagineComparison of Transverse and Vertical Skin Incision For Emergency Cesarean DeliveryGinecólogo Oncólogo Danilo Baltazar ChaconNessuna valutazione finora
- Risk and Benefit of CSDocumento22 pagineRisk and Benefit of CSbudi haryadiNessuna valutazione finora
- Breast Cancer in Young WomenDa EverandBreast Cancer in Young WomenOreste GentiliniNessuna valutazione finora
- CSP - Groin LumpDocumento39 pagineCSP - Groin LumpAnnisa SakilaNessuna valutazione finora
- Final DNB Seat Matrix For PG 2022Documento204 pagineFinal DNB Seat Matrix For PG 2022Minerva Medical Treatment Pvt LtdNessuna valutazione finora
- Composite Resin RestorationDocumento9 pagineComposite Resin RestorationSawsan Z. JwaiedNessuna valutazione finora
- A Clinical Study of Abdominal Wound DehiscenceDocumento25 pagineA Clinical Study of Abdominal Wound DehiscenceKarthikeyan RNessuna valutazione finora
- Nicu DesignDocumento27 pagineNicu DesignNITHA KNessuna valutazione finora
- ChoeDocumento116 pagineChoeJihad AnadNessuna valutazione finora
- MRCOG Short Answer Questions September 2013Documento1 paginaMRCOG Short Answer Questions September 2013Dr.Marva YusafzaiNessuna valutazione finora
- Essential Newborn Care & BreastfeedingDocumento7 pagineEssential Newborn Care & BreastfeedingDianne LabisNessuna valutazione finora
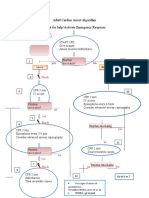
- Adult Cardiac Arrest Treatment AlgorithmDocumento1 paginaAdult Cardiac Arrest Treatment AlgorithmICU RSBMNessuna valutazione finora
- Resume and References Emily Olivia HaywardDocumento2 pagineResume and References Emily Olivia Haywardapi-349400116Nessuna valutazione finora
- Letter of Recommendation 1Documento1 paginaLetter of Recommendation 1api-405020419Nessuna valutazione finora
- Colorectal Cancer: - Dr. Suneet KhuranaDocumento36 pagineColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooNessuna valutazione finora
- Pelvic Inflammatory DiseaseDocumento3 paginePelvic Inflammatory DiseaseRania S. HamdanNessuna valutazione finora
- Aswathy P K - Resume NewDocumento3 pagineAswathy P K - Resume NewsherrymattNessuna valutazione finora
- Mcqs in Medical Physiology 2014 EspDocumento138 pagineMcqs in Medical Physiology 2014 EspdaqNessuna valutazione finora
- Internet Case For Supplement 7Documento3 pagineInternet Case For Supplement 7johnmia20Nessuna valutazione finora
- Breech Presentation: (English Case)Documento56 pagineBreech Presentation: (English Case)Heri FarnasNessuna valutazione finora
- Edan ManualDocumento14 pagineEdan ManualTony Nava100% (1)
- Patient Handover, Patient EndorsementDocumento12 paginePatient Handover, Patient Endorsementgladz25100% (2)
- Ian Stevenson Psychiatrist Who Researched ReincarnationDocumento2 pagineIan Stevenson Psychiatrist Who Researched ReincarnationJosé Antonio FranciscoNessuna valutazione finora
- NCCN Bone CancerDocumento93 pagineNCCN Bone Canceraurika sinambelaNessuna valutazione finora
- Maternity Case 7: Carla Hernandez (Core) : Guided Reflection QuestionsDocumento2 pagineMaternity Case 7: Carla Hernandez (Core) : Guided Reflection QuestionsDai Nguyen100% (1)
- Teratology Primer PDFDocumento104 pagineTeratology Primer PDFberlianromaNessuna valutazione finora
- HCP - Lists - Licensed Medical Practitioners - v1.0 - 2018Documento89 pagineHCP - Lists - Licensed Medical Practitioners - v1.0 - 2018Sam san100% (1)
- Caesarean SectionDocumento23 pagineCaesarean SectionNurul Fahmiza TumiranNessuna valutazione finora
- TolmarDocumento2 pagineTolmarKaty WohlrabNessuna valutazione finora
- S M C L: Aint Ichael'S Ollege of AgunaDocumento12 pagineS M C L: Aint Ichael'S Ollege of AgunaChriza Joy BartolomeNessuna valutazione finora
- Maternal Perception of Fetal Movements and Real-Time Ultrasound FindingsDocumento6 pagineMaternal Perception of Fetal Movements and Real-Time Ultrasound FindingsDarian AngNessuna valutazione finora
- Enhanced Recovery ProtocolsDocumento17 pagineEnhanced Recovery ProtocolsHening Tirta KusumawardaniNessuna valutazione finora
- Liver EnzymesDocumento6 pagineLiver EnzymesWande AyodeleNessuna valutazione finora