Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- What Is Breech Position?: Frank Breech. The Buttocks Are in Place To Come Out First DuringDocumento2 pagineWhat Is Breech Position?: Frank Breech. The Buttocks Are in Place To Come Out First DuringkeithevaristoNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Placenta Accreta Spectrum and Postpartum Hemorrhag - 230510 - 170158Documento10 paginePlacenta Accreta Spectrum and Postpartum Hemorrhag - 230510 - 170158Nilfacio PradoNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Stages of Labour: First StageDocumento37 pagineStages of Labour: First StageJude Martin100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Jurnal Mual MuntahDocumento4 pagineJurnal Mual MuntahMelda Sri WahyuNingsihNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- International Fetal Size Standards in Early Pregnancy: Centiles Gestational Age (Weeks + Days)Documento4 pagineInternational Fetal Size Standards in Early Pregnancy: Centiles Gestational Age (Weeks + Days)Shoaib AlamNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- BreechDocumento50 pagineBreechEldrinAbquinaNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- MCN - P2 Post Test (Reviewer)Documento3 pagineMCN - P2 Post Test (Reviewer)cianixNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- RHU III Pres ScoresDocumento15 pagineRHU III Pres ScoresFret Ramirez Coronia RNNessuna valutazione finora
- Terminologia Embryologica - 2 (FIPAT к НИР2023)Documento329 pagineTerminologia Embryologica - 2 (FIPAT к НИР2023)Sadyk MerdanowNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Toag 7 2 140 27081 PDFDocumento1 paginaToag 7 2 140 27081 PDFsaritha OrugantiNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Allen RHDocumento5 pagineAllen RHVadhilla SafitriNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
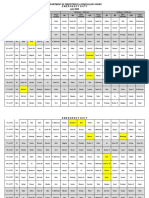
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Documento3 pagineDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Vaginal ExamDocumento24 pagineVaginal ExamschxzerrydawnNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Thyroid Dysfunction and Abnormal Uterine Bleeding: Gynecology and Women's HealthDocumento7 pagineThyroid Dysfunction and Abnormal Uterine Bleeding: Gynecology and Women's HealthnandaNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- A Woman With Placenta PreviaDocumento2 pagineA Woman With Placenta PreviaMiriam Saena EscarlosNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- MCN SF Chapter 17 QuizDocumento3 pagineMCN SF Chapter 17 QuizKathleen AngNessuna valutazione finora
- Postpartum Clinical Prep SheetDocumento3 paginePostpartum Clinical Prep SheetKurata432Nessuna valutazione finora
- Case Preterm Labor Ch.Documento29 pagineCase Preterm Labor Ch.Gazala Parveen100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Influence of Progesterone On Oocyte Quality and Embryo Development in Cows.Documento8 pagineInfluence of Progesterone On Oocyte Quality and Embryo Development in Cows.Luis MezaNessuna valutazione finora
- Maternal & Child NursingDocumento15 pagineMaternal & Child NursingLilian Flores100% (2)
- Teenage PregnancyDocumento10 pagineTeenage PregnancyKrisha Czarine Lutchiang100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- SOP IncDocumento8 pagineSOP Incsigit priyo nugrohoNessuna valutazione finora
- Malformations of Female Genital OrgansDocumento28 pagineMalformations of Female Genital OrgansTommy SinghNessuna valutazione finora
- Paediatrica Indonesiana: Original ArticleDocumento8 paginePaediatrica Indonesiana: Original ArticleNuaimatul Hani'ahNessuna valutazione finora
- Name of The Drug Mechani SM of Action Dosage Indicatio NS Contraindica Tions Adverse Reaction Nursing ResponsibilitiesDocumento2 pagineName of The Drug Mechani SM of Action Dosage Indicatio NS Contraindica Tions Adverse Reaction Nursing Responsibilitieshey aadarshaNessuna valutazione finora
- OBDocumento6 pagineOBbsn_cathNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Medical Record Prenatal and Pregnancy: Nestor Chicago J IL 60635 Kathy 333 East 3rd StreetDocumento11 pagineMedical Record Prenatal and Pregnancy: Nestor Chicago J IL 60635 Kathy 333 East 3rd StreetDerrick ThompsonNessuna valutazione finora
- 2004, Vol.31, Issues 1, Ultrasound in ObstetricsDocumento213 pagine2004, Vol.31, Issues 1, Ultrasound in ObstetricsFebrinata MahadikaNessuna valutazione finora
- Perdarahan Uterus AbnormalDocumento37 paginePerdarahan Uterus AbnormalElno Tatipikalawan100% (1)
- Infertility and ItDocumento3 pagineInfertility and ItDeepanshu ShakargayeNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)