Potrebbero piacerti anche
- Dengue Fever InfoDocumento12 pagineDengue Fever InfonqadirNessuna valutazione finora
- Filaria Tool KitDocumento64 pagineFilaria Tool KitdeepikaNessuna valutazione finora
- Dengue English ColourDocumento12 pagineDengue English ColourdeepikaNessuna valutazione finora
- Guidelines For ANM NewDocumento6 pagineGuidelines For ANM NewdeepikaNessuna valutazione finora
- P 3085Documento1 paginaP 3085Ne' GitgNessuna valutazione finora
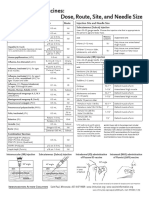
- Accination As Per The National Immunization Schedule by Government of IndiaDocumento1 paginaAccination As Per The National Immunization Schedule by Government of IndiadeepikaNessuna valutazione finora
- Plant Tissue2Documento18 paginePlant Tissue2Aman ChaudharyNessuna valutazione finora
- Air and Water PDFDocumento32 pagineAir and Water PDFdeepikaNessuna valutazione finora
- 4 Posters Promoting Community Mental Health HINDIDocumento4 pagine4 Posters Promoting Community Mental Health HINDIdeepikaNessuna valutazione finora
- Immunization Chart SuperBabyDocumento5 pagineImmunization Chart SuperBabydeepikaNessuna valutazione finora
- All Paramedical CoursesDocumento23 pagineAll Paramedical CoursesdeepikaNessuna valutazione finora
- BondingDocumento3 pagineBondingdeepikaNessuna valutazione finora
- FICCI Heal Report Final 27-08-2016Documento56 pagineFICCI Heal Report Final 27-08-2016deepikaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Curriculum Vitae: CV of Ir. Chai Seong Wai (Jobstreet 2020) Page 1 of 6Documento6 pagineCurriculum Vitae: CV of Ir. Chai Seong Wai (Jobstreet 2020) Page 1 of 6Kevin LowNessuna valutazione finora
- ProPublica MethodologyDocumento5 pagineProPublica MethodologySouthern California Public RadioNessuna valutazione finora
- Hospitall PDFDocumento2 pagineHospitall PDFPrashant WankhadeNessuna valutazione finora
- Code Blue Procedures: Luis Enriquez RN, BSDocumento25 pagineCode Blue Procedures: Luis Enriquez RN, BSmonir61100% (1)
- ST George Hospital - Neuro InpatientsDocumento2 pagineST George Hospital - Neuro InpatientsDaniel ChongNessuna valutazione finora
- History of Nursing-An OverviewDocumento5 pagineHistory of Nursing-An Overviewjava_biscocho1229100% (3)
- Standard Operating Procedure Checklist To Prevent Covid19 For Warangal Project SiteDocumento1 paginaStandard Operating Procedure Checklist To Prevent Covid19 For Warangal Project SiteImranuddin SyedNessuna valutazione finora
- Desain Form Medical RecordDocumento5 pagineDesain Form Medical RecordIbrahim ChandraNessuna valutazione finora
- Case StudyDocumento78 pagineCase StudyRAGHVENDRANessuna valutazione finora
- Laws and Rules Governing HospitalsDocumento6 pagineLaws and Rules Governing HospitalsAnil BgNessuna valutazione finora
- Data Dokter Dari GmailDocumento12 pagineData Dokter Dari GmailAlfen HFNessuna valutazione finora
- Ound TherapyDocumento14 pagineOund TherapyAndrewJohnsonJenssonNessuna valutazione finora
- Hand Washing RsDocumento4 pagineHand Washing RsChachaNessuna valutazione finora
- The Florida Mental Health Act (The Baker Act) 2000 Annual ReportDocumento54 pagineThe Florida Mental Health Act (The Baker Act) 2000 Annual ReportaptureincNessuna valutazione finora
- Fdar Lp6 MontemayorDocumento5 pagineFdar Lp6 MontemayorEden Marie MangaserNessuna valutazione finora
- Principle of ElectroDx by Dr. Angkana Nudsasarn, Chiang Mai UniversityDocumento113 paginePrinciple of ElectroDx by Dr. Angkana Nudsasarn, Chiang Mai UniversitySurat Tanprawate100% (3)
- Improving Patient Safety in The Operating Theatre and Perioperative Care: Obstacles, Interventions, and Priorities For Accelerating ProgressDocumento14 pagineImproving Patient Safety in The Operating Theatre and Perioperative Care: Obstacles, Interventions, and Priorities For Accelerating ProgressKainat BaigNessuna valutazione finora
- Medicare Part B: Highmark Medicare Services Documentation WorksheetDocumento4 pagineMedicare Part B: Highmark Medicare Services Documentation Worksheetgraylove10Nessuna valutazione finora
- Causes and Treatment Outcome of Mechanical Bowel Obstruction in North Eastern NigeriaDocumento3 pagineCauses and Treatment Outcome of Mechanical Bowel Obstruction in North Eastern NigeriakeithNessuna valutazione finora
- Republic of The Philippines Davao Oriental State College of Science and TechnologyDocumento4 pagineRepublic of The Philippines Davao Oriental State College of Science and Technologydinheadnursing09Nessuna valutazione finora
- Design 1 Plans-ModelDocumento1 paginaDesign 1 Plans-ModelKinjal HarpavatNessuna valutazione finora
- RS. Premier Bintaro Pathology Service RS. Premier Bintaro Pathology ServiceDocumento1 paginaRS. Premier Bintaro Pathology Service RS. Premier Bintaro Pathology Serviceintan riniNessuna valutazione finora
- English Drama Script in The HospitalDocumento4 pagineEnglish Drama Script in The HospitalS Yogaa Muliaa100% (1)
- General Scheme Rules For Jubilee Micro Cover 2023Documento1 paginaGeneral Scheme Rules For Jubilee Micro Cover 2023Africa Inuka Hospital UgunjaNessuna valutazione finora
- Report (Code of Ethics)Documento14 pagineReport (Code of Ethics)Chris ⏠⏝⏠ MarianoNessuna valutazione finora
- Value Based Healthcare - DR Robert KaplanDocumento43 pagineValue Based Healthcare - DR Robert KaplanArin D100% (1)
- The Burning Girl - Claire MessudDocumento104 pagineThe Burning Girl - Claire MessudNachoNessuna valutazione finora
- Test1 (1) 5Documento5 pagineTest1 (1) 5revjamesfaqirNessuna valutazione finora
- Resume: Sub: Job For The Clnical Staff NurseDocumento6 pagineResume: Sub: Job For The Clnical Staff NurseJai SinghrandhawaNessuna valutazione finora
- HTH 2012 00165Documento464 pagineHTH 2012 00165Bob MackinNessuna valutazione finora