Potrebbero piacerti anche
- Causes of Hearing LossDocumento2 pagineCauses of Hearing LossAdjei Fosu KennedyNessuna valutazione finora
- Upper Airway ObstructionDocumento31 pagineUpper Airway ObstructiontrimardiyanaisyanNessuna valutazione finora
- Properties of BloodDocumento3 pagineProperties of BloodRaj SinghNessuna valutazione finora
- Physiology & Pathophysiology of PainDocumento31 paginePhysiology & Pathophysiology of Painkuncupcupu1368Nessuna valutazione finora
- Respiratory System - Anatomy & PhysiologyDocumento24 pagineRespiratory System - Anatomy & PhysiologySarthak ShahNessuna valutazione finora
- Hearing LossDocumento31 pagineHearing LossDat boi100% (1)
- Prepared By: Edwin Jonathan A. Manlapas, DDM, R.NDocumento726 paginePrepared By: Edwin Jonathan A. Manlapas, DDM, R.NQuolette ConstanteNessuna valutazione finora
- Oral Manifestations of Nutritional Disorders2Documento33 pagineOral Manifestations of Nutritional Disorders2Yeoh Wen LiNessuna valutazione finora
- MEN1 PPDocumento15 pagineMEN1 PPAaron D. PhoenixNessuna valutazione finora
- Fluid and Electrolyte Imbalance and Nutritional ProblemDocumento98 pagineFluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerNessuna valutazione finora
- Vital Signs and TestingDocumento47 pagineVital Signs and TestingRegina Garrard100% (1)
- Tonsillectomy Slides 050427Documento62 pagineTonsillectomy Slides 050427Aidiel FikriNessuna valutazione finora
- Connective TissueDocumento13 pagineConnective TissueHelena Allguter100% (3)
- PARASYMPATHETIC GANGLIA IN HEAD AND NECKDocumento53 paginePARASYMPATHETIC GANGLIA IN HEAD AND NECKDEEP SABNessuna valutazione finora
- Surgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDocumento32 pagineSurgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDr Prashant Kumar100% (1)
- The Lymphatic System and Body Defenses: Elaine N. MariebDocumento75 pagineThe Lymphatic System and Body Defenses: Elaine N. MariebReysa ManulatNessuna valutazione finora
- Everything You Need to Know About RicketsDocumento32 pagineEverything You Need to Know About RicketsDarina Ismakaieva100% (1)
- Nutrient EssentialsDocumento37 pagineNutrient EssentialsM DNessuna valutazione finora
- 01.anatomy of The EarDocumento52 pagine01.anatomy of The EarJumanne Jay100% (1)
- Respiratory System AssessmentDocumento13 pagineRespiratory System Assessmentavinash dhameriyaNessuna valutazione finora
- Otosclerosis Slides 061018Documento96 pagineOtosclerosis Slides 061018Paraguay De La Cruz JoelNessuna valutazione finora
- NEUROMUSCULAR TRANSMISSION: ANATOMY AND PHYSIOLOGYDocumento45 pagineNEUROMUSCULAR TRANSMISSION: ANATOMY AND PHYSIOLOGYparuNessuna valutazione finora
- Ear DisordersDocumento7 pagineEar DisordersGéorel John Colonia GoteraNessuna valutazione finora
- Physiology of Hearing: Departemen Fisiologi FK UsuDocumento28 paginePhysiology of Hearing: Departemen Fisiologi FK UsuSonia P SNessuna valutazione finora
- Pathogenesis of Hearing Loss ExplainedDocumento6 paginePathogenesis of Hearing Loss ExplainedYogi HadityaNessuna valutazione finora
- Thalassemia: Dr. Deep Shah Under Guidance of Dr. Krutika Ma'Am and Dr. Rahul SirDocumento46 pagineThalassemia: Dr. Deep Shah Under Guidance of Dr. Krutika Ma'Am and Dr. Rahul SirDeep ShahNessuna valutazione finora
- INTUSSUSCEPTIONDocumento3 pagineINTUSSUSCEPTIONS GNessuna valutazione finora
- CANINE-Spontaneous Pneumothorax in DogsDocumento7 pagineCANINE-Spontaneous Pneumothorax in Dogstaner_soysurenNessuna valutazione finora
- Chronic Suppurative Otitis MediaDocumento27 pagineChronic Suppurative Otitis MediaJoshua JayakaranNessuna valutazione finora
- Anatomy and Physiology ReviewerDocumento52 pagineAnatomy and Physiology ReviewerCourtney Dela FierraNessuna valutazione finora
- Ass - Prof. Dr. Saif Ali Ahmed GhabishaDocumento103 pagineAss - Prof. Dr. Saif Ali Ahmed Ghabishaalina nguynNessuna valutazione finora
- Physiology of BalanceDocumento27 paginePhysiology of Balancemulkihakam21Nessuna valutazione finora
- Chromosomal AbnormalitiesDocumento6 pagineChromosomal AbnormalitiesPrashant MundeNessuna valutazione finora
- Skeletal SystemDocumento32 pagineSkeletal SystemMatthew HallNessuna valutazione finora
- Stomach Peptic UlcerDocumento38 pagineStomach Peptic UlcermohamedNessuna valutazione finora
- Tissue CultureDocumento44 pagineTissue Culturebioenviron100% (1)
- Development of HeartDocumento15 pagineDevelopment of Heartash ashNessuna valutazione finora
- Introduction To Pathology: Sunilkumar.P Haematology & Transfusion Medicine ST - John's Medical College Hospital BangaloreDocumento39 pagineIntroduction To Pathology: Sunilkumar.P Haematology & Transfusion Medicine ST - John's Medical College Hospital BangalorefahdabdNessuna valutazione finora
- Final Anatomy Exam Questions PRE MED: Yara AdeebDocumento3 pagineFinal Anatomy Exam Questions PRE MED: Yara AdeebMadani TawfeeqNessuna valutazione finora
- Uk PFAPADocumento5 pagineUk PFAPAPrerna SehgalNessuna valutazione finora
- ANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaDocumento36 pagineANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaBonieve Pitogo NoblezadaNessuna valutazione finora
- OxygenationDocumento57 pagineOxygenationassumptaNessuna valutazione finora
- 1.acute PharyngitisDocumento88 pagine1.acute PharyngitisIhsan Hanif0% (1)
- BotulismDocumento2 pagineBotulismAdrian MangahasNessuna valutazione finora
- AneurysmDocumento6 pagineAneurysmJozelle PhilipNessuna valutazione finora
- ArthritisDocumento18 pagineArthritisGEETA MOHAN100% (1)
- Chapter 13 Student Version The Respiratory System 2020.ppt (1186)Documento18 pagineChapter 13 Student Version The Respiratory System 2020.ppt (1186)S. MartinezNessuna valutazione finora
- Anatomy and Physiology of Adrenal GlandDocumento26 pagineAnatomy and Physiology of Adrenal GlandYAMINIPRIYANNessuna valutazione finora
- AerosolsDocumento9 pagineAerosolsTubaNessuna valutazione finora
- Perichondritis PinnaDocumento2 paginePerichondritis PinnaAnish RajNessuna valutazione finora
- Clinical Assessment of Hearing With Free Field Voice Testing and Tuning Forks PDFDocumento11 pagineClinical Assessment of Hearing With Free Field Voice Testing and Tuning Forks PDFRodolfo Eduardo Garnica FernandezNessuna valutazione finora
- Martha Rogers: Presented By: Lyndsi Byers, Geena Griffin, Chelsea Hoy and Mallory ShepardDocumento18 pagineMartha Rogers: Presented By: Lyndsi Byers, Geena Griffin, Chelsea Hoy and Mallory ShepardChelsea Hoy100% (2)
- 04 & 05 - InflamationDocumento31 pagine04 & 05 - InflamationAdarshBijapur100% (1)
- Causes and Management of Syncope in DentistryDocumento27 pagineCauses and Management of Syncope in DentistrySelvarathi KandhaswamyNessuna valutazione finora
- New Vertin CME Slides FinalDocumento98 pagineNew Vertin CME Slides FinalGaurav KatariaNessuna valutazione finora
- BMED 3107 Endocrine & Reproductive Systems DevelopmentDocumento32 pagineBMED 3107 Endocrine & Reproductive Systems DevelopmentMarisol AcostaNessuna valutazione finora
- Veterinary Obstetrics IntroductionDocumento27 pagineVeterinary Obstetrics IntroductionShakil MahmodNessuna valutazione finora
- Lab Report 1. Tissues: Fig. 1: Mammal Artery and Vein - Cross SectionDocumento11 pagineLab Report 1. Tissues: Fig. 1: Mammal Artery and Vein - Cross Sectionapi-3798860100% (5)
- Tumours of Larynx: A Clinicopathological StudyDa EverandTumours of Larynx: A Clinicopathological StudyNessuna valutazione finora
- Anatomy and Physiology Terms: Brief Definitions, Roots & Morphology; An Abecedary; Vol 10 - Digestive System TermsDa EverandAnatomy and Physiology Terms: Brief Definitions, Roots & Morphology; An Abecedary; Vol 10 - Digestive System TermsNessuna valutazione finora
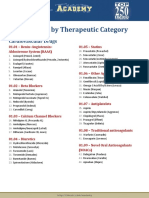
- Drug List by Therapeutic Category: Cardiovascular DrugsDocumento7 pagineDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Nessuna valutazione finora
- Pharmacological Classification of Drugs First EditionDocumento22 paginePharmacological Classification of Drugs First EditionAsiya ZaidiNessuna valutazione finora
- Pharmacological Classification of Drugs First EditionDocumento0 paginePharmacological Classification of Drugs First EditionAmina BećiragićNessuna valutazione finora
- 0194599812467004Documento55 pagine0194599812467004Asiya ZaidiNessuna valutazione finora
- List of Drugs PDFDocumento59 pagineList of Drugs PDFLouriel Nopal100% (1)
- List of Books - Pharmacology TitlesDocumento2 pagineList of Books - Pharmacology TitlesAsiya ZaidiNessuna valutazione finora
- CI ComparisonDocumento7 pagineCI ComparisonAsiya ZaidiNessuna valutazione finora
- 0194599812467004Documento55 pagine0194599812467004Asiya ZaidiNessuna valutazione finora
- 100 Cases in Ear, Nose & ThroatDocumento45 pagine100 Cases in Ear, Nose & Throatapi-3730930100% (17)
- Myringoplasty and TympanoplastyDocumento20 pagineMyringoplasty and TympanoplastyAsiya Zaidi100% (1)
- Foreign Body AspirationDocumento3 pagineForeign Body AspirationAsiya ZaidiNessuna valutazione finora
- Cholesteatoma Pic 2013 05Documento90 pagineCholesteatoma Pic 2013 05Asiya ZaidiNessuna valutazione finora
- Facial Paral Pic 2012 10 BDocumento70 pagineFacial Paral Pic 2012 10 BAsiya ZaidiNessuna valutazione finora
- Reconstruction of Middle Ear CavityDocumento56 pagineReconstruction of Middle Ear CavityAsiya ZaidiNessuna valutazione finora
- Cranial Nerve Examination For Neurogenic Dysphagia Patients 2161 119X 1000319Documento6 pagineCranial Nerve Examination For Neurogenic Dysphagia Patients 2161 119X 1000319Asiya ZaidiNessuna valutazione finora
- Ossicular Recon Slides 090629Documento89 pagineOssicular Recon Slides 090629Mohammed Sahib100% (1)
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDocumento9 pagineOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryAsiya ZaidiNessuna valutazione finora
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDocumento9 pagineOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryAsiya ZaidiNessuna valutazione finora
- Mastoidectomy and EpitympanectomyDocumento18 pagineMastoidectomy and EpitympanectomyAsiya ZaidiNessuna valutazione finora
- Hoarse Lesion Slides 090306Documento61 pagineHoarse Lesion Slides 090306Asiya ZaidiNessuna valutazione finora
- Occlusion For Implant Suppported CDDocumento4 pagineOcclusion For Implant Suppported CDpopat78Nessuna valutazione finora
- Labcorp: Patient ReportDocumento4 pagineLabcorp: Patient ReportAsad PrinceNessuna valutazione finora
- Nursing Assessment 1Documento70 pagineNursing Assessment 1Amira AttyaNessuna valutazione finora
- Sdera Demo Lesson DVD Worksheet 2021Documento2 pagineSdera Demo Lesson DVD Worksheet 2021api-396577001Nessuna valutazione finora
- Occipital LobesDocumento46 pagineOccipital LobesLakshya J Basumatary100% (1)
- Perioperative NursingDocumento8 paginePerioperative NursingGil Platon Soriano100% (3)
- Science of 7 ChakraDocumento6 pagineScience of 7 ChakraSheebaNessuna valutazione finora
- (260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPDocumento43 pagine(260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPreginaNessuna valutazione finora
- Swollen Feet During PregnancyDocumento2 pagineSwollen Feet During PregnancyDede YasminNessuna valutazione finora
- A Harmonious Smile: Biological CostsDocumento12 pagineA Harmonious Smile: Biological Costsjsjs kaknsbsNessuna valutazione finora
- 7 Steps To The Perfect PICO Search White PaperDocumento9 pagine7 Steps To The Perfect PICO Search White PaperNurkhasanah 71Nessuna valutazione finora
- Workplace EmergenciesDocumento39 pagineWorkplace EmergenciesUpul Nishantha ThalpawilaNessuna valutazione finora
- Prevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDDocumento7 paginePrevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDMusainah FeisalNessuna valutazione finora
- MalariaDocumento11 pagineMalariaWynli Fullo AncogNessuna valutazione finora
- A Case of Eclectic Family TherapyDocumento88 pagineA Case of Eclectic Family Therapygun gorNessuna valutazione finora
- Legalizing abortion in the Philippines for women's health and rightsDocumento2 pagineLegalizing abortion in the Philippines for women's health and rightsRosario Antoniete R. Cabilin100% (1)
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Documento10 pagineAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNessuna valutazione finora
- October 2022 Complete Month CA English - CompressedDocumento117 pagineOctober 2022 Complete Month CA English - CompressedKing JNessuna valutazione finora
- NHS Trust PolicyDocumento52 pagineNHS Trust Policyver_at_workNessuna valutazione finora
- Spartan Bodyweight WorkoutsDocumento102 pagineSpartan Bodyweight WorkoutsSamir DjoudiNessuna valutazione finora
- 4bi1 - Jan22 2b QPDocumento28 pagine4bi1 - Jan22 2b QPXIN PEINessuna valutazione finora
- Strupp ArticleDocumento10 pagineStrupp ArticleDental SpaNessuna valutazione finora
- "PASS" Principles For Predictable PDFDocumento10 pagine"PASS" Principles For Predictable PDFkishan bordaNessuna valutazione finora
- Dat IatDocumento4 pagineDat Iatscribd birdNessuna valutazione finora
- Qatar Healthcare Facilities Contact GuideDocumento3 pagineQatar Healthcare Facilities Contact GuideShibu KavullathilNessuna valutazione finora
- Part A Reading Task Playground Injuries Playground Surface MaterialDocumento8 paginePart A Reading Task Playground Injuries Playground Surface MaterialMitra NabizadehNessuna valutazione finora
- Drug StudyDocumento11 pagineDrug StudyHennah Reblando100% (3)
- Rosemont Hill Health CenterDocumento14 pagineRosemont Hill Health CenterMona SahooNessuna valutazione finora
- Tradition With A Future: Solutions For Operative HysterosDocumento16 pagineTradition With A Future: Solutions For Operative Hysterosأحمد قائدNessuna valutazione finora
- OCPD: Symptoms, Diagnosis and TreatmentDocumento4 pagineOCPD: Symptoms, Diagnosis and TreatmentRana Muhammad Ahmad Khan ManjNessuna valutazione finora