Potrebbero piacerti anche
- (Journals) Proposals For Paraphilic Disorders in The International PDFDocumento17 pagine(Journals) Proposals For Paraphilic Disorders in The International PDFD'esika Han ChanNessuna valutazione finora
- (Journal) Sexual Sadism and The Psychopathy Facets As Predictors ofDocumento49 pagine(Journal) Sexual Sadism and The Psychopathy Facets As Predictors ofD'esika Han ChanNessuna valutazione finora
- (Journals) Profiles and Sexual Practices of Current and PastDocumento5 pagine(Journals) Profiles and Sexual Practices of Current and PastD'esika Han ChanNessuna valutazione finora
- Sadism Articlecjp Oct 08 Federoff IRDocumento11 pagineSadism Articlecjp Oct 08 Federoff IRmiftah_wahyudi100% (1)
- (Journals) Modelling of The Sadomasokisme PDFDocumento23 pagine(Journals) Modelling of The Sadomasokisme PDFD'esika Han ChanNessuna valutazione finora
- The Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorDocumento11 pagineThe Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorMichael Tavera OsorioNessuna valutazione finora
- (Journals) BDSM Disclosure and Stigma Management PDFDocumento25 pagine(Journals) BDSM Disclosure and Stigma Management PDFD'esika Han ChanNessuna valutazione finora
- (Journals) Proposals For Paraphilic Disorders in The International PDFDocumento17 pagine(Journals) Proposals For Paraphilic Disorders in The International PDFD'esika Han ChanNessuna valutazione finora
- (Journals) BDSM Disclosure and Stigma Management PDFDocumento25 pagine(Journals) BDSM Disclosure and Stigma Management PDFD'esika Han ChanNessuna valutazione finora
- The Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorDocumento11 pagineThe Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorMichael Tavera OsorioNessuna valutazione finora
- (Journals) Modelling of The Sadomasokisme PDFDocumento23 pagine(Journals) Modelling of The Sadomasokisme PDFD'esika Han ChanNessuna valutazione finora
- (Journals) Profiles and Sexual Practices of Current and PastDocumento5 pagine(Journals) Profiles and Sexual Practices of Current and PastD'esika Han ChanNessuna valutazione finora
- Positive Bacterial Culture in Conjunctival SacDocumento5 paginePositive Bacterial Culture in Conjunctival SacD'esika Han ChanNessuna valutazione finora
- Effectiveness of Nonpharmacologic Treatments For Acute Seasonal Allergic ConjunctivitisDocumento7 pagineEffectiveness of Nonpharmacologic Treatments For Acute Seasonal Allergic ConjunctivitisMas Teguh WijayantoNessuna valutazione finora
- The Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorDocumento11 pagineThe Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorMichael Tavera OsorioNessuna valutazione finora
- Effectiveness of Nonpharmacologic Treatments For Acute Seasonal Allergic ConjunctivitisDocumento7 pagineEffectiveness of Nonpharmacologic Treatments For Acute Seasonal Allergic ConjunctivitisMas Teguh WijayantoNessuna valutazione finora
- Positive Bacterial Culture in Conjunctival SacDocumento5 paginePositive Bacterial Culture in Conjunctival SacD'esika Han ChanNessuna valutazione finora
- Conjunctival Microbiome Changes Associated With SoftDocumento9 pagineConjunctival Microbiome Changes Associated With SoftD'esika Han ChanNessuna valutazione finora
- The Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorDocumento11 pagineThe Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorMichael Tavera OsorioNessuna valutazione finora
- Effectiveness of Nonpharmacologic Treatments For Acute Seasonal Allergic ConjunctivitisDocumento7 pagineEffectiveness of Nonpharmacologic Treatments For Acute Seasonal Allergic ConjunctivitisMas Teguh WijayantoNessuna valutazione finora
- Conjunctival Microangiopathy in A Patient With Neovascular GlaucomaDocumento7 pagineConjunctival Microangiopathy in A Patient With Neovascular GlaucomaD'esika Han ChanNessuna valutazione finora
- (Journal) Sexual Sadism and The Psychopathy Facets As Predictors ofDocumento49 pagine(Journal) Sexual Sadism and The Psychopathy Facets As Predictors ofD'esika Han ChanNessuna valutazione finora
- (Journals) BDSM Disclosure and Stigma Management PDFDocumento25 pagine(Journals) BDSM Disclosure and Stigma Management PDFD'esika Han ChanNessuna valutazione finora
- (Journals) BDSM Disclosure and Stigma Management PDFDocumento25 pagine(Journals) BDSM Disclosure and Stigma Management PDFD'esika Han ChanNessuna valutazione finora
- (Journal) Sexual Sadism and The Psychopathy Facets As Predictors ofDocumento49 pagine(Journal) Sexual Sadism and The Psychopathy Facets As Predictors ofD'esika Han ChanNessuna valutazione finora
- Sadism Articlecjp Oct 08 Federoff IRDocumento11 pagineSadism Articlecjp Oct 08 Federoff IRmiftah_wahyudi100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- NCP Glaukoma Dan KatarakDocumento1 paginaNCP Glaukoma Dan KatarakIsmi Nur KhikmahNessuna valutazione finora
- What Is Visual Disturbance?: Retinal or Ocular MigraineDocumento14 pagineWhat Is Visual Disturbance?: Retinal or Ocular MigraineJesusNessuna valutazione finora
- Rockaway Times 8416Documento48 pagineRockaway Times 8416Peter J. MahonNessuna valutazione finora
- Enhancement and Feature Extraction of Fundus ImagesDocumento5 pagineEnhancement and Feature Extraction of Fundus ImagesInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Interpreting Automated Perimetry - B - Thomas Ravi, George Ronn..Documento28 pagineInterpreting Automated Perimetry - B - Thomas Ravi, George Ronn..Sarah KemalasariNessuna valutazione finora
- Ijo 08 01 081Documento8 pagineIjo 08 01 081Pretty ClarresaNessuna valutazione finora
- 20-20-20 Rule To Prevent Eye StrainDocumento9 pagine20-20-20 Rule To Prevent Eye StrainNazifa HelfiNessuna valutazione finora
- Strabismus PDFDocumento170 pagineStrabismus PDFShari Ali100% (1)
- Best Aid To Ophthalmology - Pramod TK - 318Documento3 pagineBest Aid To Ophthalmology - Pramod TK - 318Danielle SangalangNessuna valutazione finora
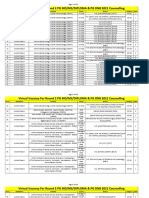
- Virtual Vacancy For Round 2 PG 2021 CounsellingDocumento355 pagineVirtual Vacancy For Round 2 PG 2021 Counsellingkrish vjNessuna valutazione finora
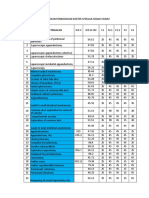
- Penggolongan OperasiDocumento32 paginePenggolongan OperasiKARTIKANessuna valutazione finora
- UVEITIS ESSENTIALSeditDocumento38 pagineUVEITIS ESSENTIALSeditSatria WidyatamaNessuna valutazione finora
- Case Study Dr. Sisk LCA Gene Therapy MC 0005054 21NOV2022Documento6 pagineCase Study Dr. Sisk LCA Gene Therapy MC 0005054 21NOV2022SALAH YOUNISNessuna valutazione finora
- Perbedaan Smile Lasik PRK 1Documento4 paginePerbedaan Smile Lasik PRK 1amandaNessuna valutazione finora
- Difference Between An OphthalmologistDocumento2 pagineDifference Between An OphthalmologistAljhon DelfinNessuna valutazione finora
- What Is A Pinguecula and A PterygiumDocumento5 pagineWhat Is A Pinguecula and A PterygiumandrewNessuna valutazione finora
- Parts of The Human Eye With DefinitionDocumento4 pagineParts of The Human Eye With DefinitionStarsky Allence Puyoc0% (1)
- Eye Exercise FAQDocumento59 pagineEye Exercise FAQCaroline BrandtNessuna valutazione finora
- Survey Ophthalmology 12 2016 Vogt-Koyanagi-Harada Disease - CompressedDocumento25 pagineSurvey Ophthalmology 12 2016 Vogt-Koyanagi-Harada Disease - CompressedCrypto UpdateNessuna valutazione finora
- Corneal and Conjunctival DegenerationsDocumento20 pagineCorneal and Conjunctival DegenerationsOnur TemizsoyluNessuna valutazione finora
- Contact Lens-Induced Limbal Stem Cell Deficiency - EyeWikiDocumento4 pagineContact Lens-Induced Limbal Stem Cell Deficiency - EyeWikiSania NadianisaNessuna valutazione finora
- Eidon - Atlas Catalog WebDocumento51 pagineEidon - Atlas Catalog Webefze71Nessuna valutazione finora
- Laser Peripheral Iridotomy: January 2005Documento5 pagineLaser Peripheral Iridotomy: January 2005Fapuw ParawansaNessuna valutazione finora
- Case Report Diabetic Retinopaty in EnglishDocumento13 pagineCase Report Diabetic Retinopaty in Englishsasha anka DilanNessuna valutazione finora
- Ophthalmology Vision Test PowerPoint TemplatesDocumento48 pagineOphthalmology Vision Test PowerPoint TemplatesEvaNessuna valutazione finora
- CataractDocumento5 pagineCataractcarls burg a. resurreccionNessuna valutazione finora
- Laban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byDocumento40 pagineLaban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byKool Kaish100% (1)
- TrachomaDocumento6 pagineTrachomaSpislgal PhilipNessuna valutazione finora
- CASE REPORT - Docx Formative Case - DocxxxxxxxxxDocumento8 pagineCASE REPORT - Docx Formative Case - DocxxxxxxxxxNismaSeharNessuna valutazione finora
- Patient Education - Allergic Conjunctivitis (Beyond The Basics) - UpToDateDocumento8 paginePatient Education - Allergic Conjunctivitis (Beyond The Basics) - UpToDateRadu BalanNessuna valutazione finora