Potrebbero piacerti anche
- Cover LetterDocumento1 paginaCover Lettermiaaudina72Nessuna valutazione finora
- Leaflet WahamDocumento2 pagineLeaflet Wahammiaaudina72Nessuna valutazione finora
- Lung Cancers: Cause ForDocumento19 pagineLung Cancers: Cause Formiaaudina72Nessuna valutazione finora
- Role Play English Language Pediatric Nursing of DHF DiseaseDocumento1 paginaRole Play English Language Pediatric Nursing of DHF Diseasemiaaudina72Nessuna valutazione finora
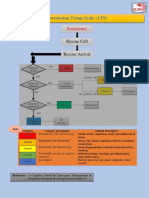
- Australasian Triage Scale (ATS) : EmergencyDocumento2 pagineAustralasian Triage Scale (ATS) : Emergencymiaaudina72Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Autoimmune Abnormalities of Postpartum Thyroid DiseasesDocumento8 pagineAutoimmune Abnormalities of Postpartum Thyroid DiseasesIpan MahendriyansaNessuna valutazione finora
- Cedar Crest College Clinical and Concept Map Worksheet For Nursing 330 PediatricsDocumento13 pagineCedar Crest College Clinical and Concept Map Worksheet For Nursing 330 Pediatricsapi-405374041Nessuna valutazione finora
- Proof Christ Was Really KundaliniDocumento3 pagineProof Christ Was Really KundaliniSevan Bomar95% (42)
- امتحان سنة ثالثة 2023Documento15 pagineامتحان سنة ثالثة 2023Dr-Mohammad Ali-Fayiz Al TamimiNessuna valutazione finora
- IM-Module B Summarized Notes (IBD)Documento69 pagineIM-Module B Summarized Notes (IBD)DeepbluexNessuna valutazione finora
- Binomial Distribution ExercisesDocumento3 pagineBinomial Distribution ExercisesAlp Eren AKYUZNessuna valutazione finora
- Sabutamol SalbutamolDocumento2 pagineSabutamol SalbutamolAnanda Felton FalconNessuna valutazione finora
- Management of PcuDocumento30 pagineManagement of Pcuapi-3698227Nessuna valutazione finora
- Npte Exam TablesDocumento586 pagineNpte Exam TablesarbazNessuna valutazione finora
- Research Paper Herbal MedicineDocumento4 pagineResearch Paper Herbal Medicineaflbtlzaw100% (1)
- CVBD Easy-To-Digest No 4 BabesiosisDocumento12 pagineCVBD Easy-To-Digest No 4 BabesiosisDocNessuna valutazione finora
- Cuscuta AssignmentDocumento12 pagineCuscuta AssignmentAshfaq Hussain KharalNessuna valutazione finora
- Annotated BibliographyDocumento3 pagineAnnotated Bibliographyapi-272471717Nessuna valutazione finora
- Hiv NotesDocumento82 pagineHiv Notesjacinta ndishNessuna valutazione finora
- NY B19 Misc FDR - WTC Disaster Response - NYCDOH - 9-12-01Documento87 pagineNY B19 Misc FDR - WTC Disaster Response - NYCDOH - 9-12-019/11 Document Archive100% (2)
- SOSCG 6jul2013 v5Documento32 pagineSOSCG 6jul2013 v5Suhazeli Abdullah100% (2)
- VirologyDocumento27 pagineVirologyAgus Nurul HidayahNessuna valutazione finora
- 27 Auramine Staining FinDocumento11 pagine27 Auramine Staining FinRahmat Sayyid ZharfanNessuna valutazione finora
- (Routledge Research in Intellectual Property) Olasupo Ayodeji Owoeye - Intellectual Property and Access To Medicines in Africa - A Regional Framework For Access-Routledge (2019)Documento291 pagine(Routledge Research in Intellectual Property) Olasupo Ayodeji Owoeye - Intellectual Property and Access To Medicines in Africa - A Regional Framework For Access-Routledge (2019)Rajnia RodriguesNessuna valutazione finora
- Jrsocmed00158 0011 PDFDocumento6 pagineJrsocmed00158 0011 PDFWahyu SutrisnaNessuna valutazione finora
- How A Diagnosis of Asperger's Transformed A Marriage: The Journal of Best Practices by David FinchDocumento24 pagineHow A Diagnosis of Asperger's Transformed A Marriage: The Journal of Best Practices by David FinchSimon and Schuster100% (10)
- Baicapil™Documento26 pagineBaicapil™HarmonyLife100% (6)
- Patofisiologi Kanker RahimDocumento98 paginePatofisiologi Kanker RahimOjo Nesu100% (1)
- Hain GenoType Line Probe Assay TestDocumento20 pagineHain GenoType Line Probe Assay Testpacome abdulNessuna valutazione finora
- Blast Injuries & Gunshot WoundsDocumento93 pagineBlast Injuries & Gunshot WoundsdocpreetiNessuna valutazione finora
- Ulcerative ColitisDocumento30 pagineUlcerative ColitisAndika SulistianNessuna valutazione finora
- Management of PPHDocumento24 pagineManagement of PPHMutabazi SharifNessuna valutazione finora
- ACEMAC 2019 BrochureDocumento5 pagineACEMAC 2019 BrochureAshley PrescottNessuna valutazione finora
- Novel p53 Splicing Site Mutation in Li-Fraumeni-like Syndrome With OsteosarcomaDocumento5 pagineNovel p53 Splicing Site Mutation in Li-Fraumeni-like Syndrome With OsteosarcomaMissy MishaNessuna valutazione finora
- Spondylolisthesis PDFDocumento121 pagineSpondylolisthesis PDFishak_alsophNessuna valutazione finora