Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- GF-304CR Dossier.Documento35 pagineGF-304CR Dossier.suria qaqcNessuna valutazione finora
- A Research Project Submitted To The: DR - Naga Rathna SupriyaDocumento6 pagineA Research Project Submitted To The: DR - Naga Rathna Supriyamansi bodaNessuna valutazione finora
- Astm B 366Documento13 pagineAstm B 366AVINASH CHAVANNessuna valutazione finora
- Evamarine: Drying Time Set-To-Touch Hard Dry Painting Interval Min MaxDocumento1 paginaEvamarine: Drying Time Set-To-Touch Hard Dry Painting Interval Min MaxcelescopitoNessuna valutazione finora
- Aldehyde, Ketones and Carboxylic AcidDocumento1 paginaAldehyde, Ketones and Carboxylic AcidGargi PathakNessuna valutazione finora
- Mil STD 650Documento210 pagineMil STD 650Roberto Carlos Cabana Orellana100% (1)
- PS-08 Painting System MSDSDocumento20 paginePS-08 Painting System MSDSGiorgi KOGOSHVILINessuna valutazione finora
- Effect of Irrigation and Stainless Steel Drills On Dental Implant Bed Heat GenerationDocumento10 pagineEffect of Irrigation and Stainless Steel Drills On Dental Implant Bed Heat GenerationIsabel XochihuaNessuna valutazione finora
- Bioscrn PDFDocumento69 pagineBioscrn PDFNicolas CancioNessuna valutazione finora
- ZL 440 Product Data SheetDocumento3 pagineZL 440 Product Data SheetVishal ChudasamaNessuna valutazione finora
- Prospectus Syllabus: Post Graduate Diploma Course in Food Analysis and Quality AssuranceDocumento19 pagineProspectus Syllabus: Post Graduate Diploma Course in Food Analysis and Quality Assurancepriyanka thapliyal100% (1)
- Bolt Torque Calculation For Girth Flange (Ref.: Dennis Moss Procedure 2-10)Documento2 pagineBolt Torque Calculation For Girth Flange (Ref.: Dennis Moss Procedure 2-10)Manoj MulikNessuna valutazione finora
- Behavior DS MM247LC (Bae2001)Documento6 pagineBehavior DS MM247LC (Bae2001)Alex CostaNessuna valutazione finora
- Nippon Muki Catalogue (Seperator Type, J-Model)Documento20 pagineNippon Muki Catalogue (Seperator Type, J-Model)Hou HonNessuna valutazione finora
- Icml Mla IDocumento3 pagineIcml Mla IDeepak100% (1)
- Chemistry Revision Guide For IGCSE Coordinated Science Chemistry Revision Guide For IGCSE Coordinated ScienceDocumento20 pagineChemistry Revision Guide For IGCSE Coordinated Science Chemistry Revision Guide For IGCSE Coordinated SciencekarlabrooksNessuna valutazione finora
- Phy Cet Wei 23Documento4 paginePhy Cet Wei 23endtimes066xNessuna valutazione finora
- Thermoelectric Cooling ModulesDocumento8 pagineThermoelectric Cooling ModuleshabteabNessuna valutazione finora
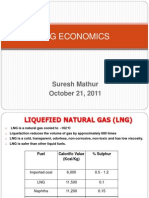
- LNG EconomicsDocumento19 pagineLNG EconomicsCal67% (3)
- NIST-JANAF Thermochemical TablesDocumento39 pagineNIST-JANAF Thermochemical TablesVelzaeroNessuna valutazione finora
- Space WeatherDocumento36 pagineSpace WeatherMat MinNessuna valutazione finora
- GelDoc XR Sole Source SpecificationsDocumento3 pagineGelDoc XR Sole Source SpecificationsdnajenNessuna valutazione finora
- Watford 2001Documento7 pagineWatford 2001CARDIO 2019Nessuna valutazione finora
- KIMO HQ210 BrochureDocumento4 pagineKIMO HQ210 BrochurebolsjhevikNessuna valutazione finora
- Beta OxidationDocumento41 pagineBeta Oxidationguna sundariNessuna valutazione finora
- High Quality Line Fi Lter Elements For All Your Fi Ltration NeedsDocumento2 pagineHigh Quality Line Fi Lter Elements For All Your Fi Ltration NeedsNuc LeusNessuna valutazione finora
- 1 2Documento65 pagine1 2AQEESHA NUWAIRA BINTI USMAN BN21110154Nessuna valutazione finora
- Consolidation Theories of Soils: By: Alemayehu Teferra (Prof., Dr.-Ing.)Documento33 pagineConsolidation Theories of Soils: By: Alemayehu Teferra (Prof., Dr.-Ing.)ASAMENEWNessuna valutazione finora
- Nutritional GSO PDFDocumento14 pagineNutritional GSO PDFjacky786Nessuna valutazione finora
- (SSOP) : Sanitation Standard Operating ProcedureDocumento6 pagine(SSOP) : Sanitation Standard Operating ProcedureAsrel05100% (1)