Potrebbero piacerti anche
- Manual FMEA 4edDocumento151 pagineManual FMEA 4edLayonAvila100% (3)
- Teste Pré-DislexiaDocumento19 pagineTeste Pré-Dislexiapatrícia nardaci100% (8)
- Livro de LógicaDocumento10 pagineLivro de LógicaPaulo Scofield50% (2)
- 13 Disfagia Valvula de FalaDocumento11 pagine13 Disfagia Valvula de FalaVivi7189Nessuna valutazione finora
- Apostila Consciência Fonológica - Jogos, Brincadeiras e AtividadesDocumento26 pagineApostila Consciência Fonológica - Jogos, Brincadeiras e AtividadesCida Macaúbas100% (23)
- Apostila Consciência Fonológica - Jogos, Brincadeiras e AtividadesDocumento26 pagineApostila Consciência Fonológica - Jogos, Brincadeiras e AtividadesCida Macaúbas100% (23)
- 3 Protocolodoperfildafluênciadafala (ABFWC)Documento1 pagina3 Protocolodoperfildafluênciadafala (ABFWC)Richard Lima OficialNessuna valutazione finora
- 04 - Deglutição AtípicaDocumento48 pagine04 - Deglutição Atípicasandrmr100% (1)
- PFPFDocumento4 paginePFPFalves_martac100% (1)
- Avaliação Fonologia ABFWDocumento1 paginaAvaliação Fonologia ABFWAndréa Garcia50% (2)
- Cartillha Discalculia PDFDocumento9 pagineCartillha Discalculia PDFRobson BatistaNessuna valutazione finora
- Cartillha Discalculia PDFDocumento9 pagineCartillha Discalculia PDFRobson BatistaNessuna valutazione finora
- Hidráulica IDocumento5 pagineHidráulica IRonnie HatfieldNessuna valutazione finora
- EdFísica 9ano Aula03Documento24 pagineEdFísica 9ano Aula03JAIRONessuna valutazione finora
- Gageira InfantilDocumento18 pagineGageira InfantilDea Matos100% (1)
- Acompanhamento longitudinal do desenvolvimento físico, cognitivo, auditivo e de linguagem da criança egressa de UTI Neonatal: contribuições da enfermagem inserida em equipe interdisciplinarDa EverandAcompanhamento longitudinal do desenvolvimento físico, cognitivo, auditivo e de linguagem da criança egressa de UTI Neonatal: contribuições da enfermagem inserida em equipe interdisciplinarNessuna valutazione finora
- ABRA GAGUEIRA - Associação Brasileira de GagueiraDocumento5 pagineABRA GAGUEIRA - Associação Brasileira de GagueiraTainá CristinnaNessuna valutazione finora
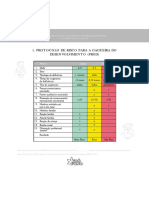
- Protocolo de Risco para A Gagueira Do Desenvolvimento (PRGD)Documento1 paginaProtocolo de Risco para A Gagueira Do Desenvolvimento (PRGD)Nicole LarissaNessuna valutazione finora
- Nota Técnica - Protocolo BristolDocumento12 pagineNota Técnica - Protocolo BristolbraddhallettNessuna valutazione finora
- Tese Gagueira UNIFESPDocumento143 pagineTese Gagueira UNIFESPTayara NascimentoNessuna valutazione finora
- PROJETO Gagueira InfantilDocumento13 paginePROJETO Gagueira InfantilSilvia Maria100% (1)
- Av LGM Bebes 0 A 3 MesesDocumento47 pagineAv LGM Bebes 0 A 3 MesesTaynara LealNessuna valutazione finora
- Consciência FonoarticulatóriaDocumento99 pagineConsciência FonoarticulatóriaLeonardoVaz100% (1)
- Discriminação Auditiva de Pares MínimosDocumento2 pagineDiscriminação Auditiva de Pares MínimosSarah FerrazNessuna valutazione finora
- AtividadeFonemaP 2 AlinefontesfonoDocumento6 pagineAtividadeFonemaP 2 AlinefontesfonoCrysline CarvalhoNessuna valutazione finora
- Articulação FonemaDocumento7 pagineArticulação FonemaStefyson BragaNessuna valutazione finora
- Anamnese Deglutição para AdultosDocumento2 pagineAnamnese Deglutição para AdultosIzabela MendesNessuna valutazione finora
- Avaliação de DisfemiaDocumento7 pagineAvaliação de DisfemiaIzabela Mendes100% (1)
- Protocolos de Avaliação Vocal UfsDocumento10 pagineProtocolos de Avaliação Vocal UfsEmilyNessuna valutazione finora
- 2015 Marchesan e Martinelli - A Fala Nos Diversos Contextos Da Motricidade Orofacial ABRAMO Cap 1 p15-28Documento13 pagine2015 Marchesan e Martinelli - A Fala Nos Diversos Contextos Da Motricidade Orofacial ABRAMO Cap 1 p15-28Mariangel CamposNessuna valutazione finora
- A Fonoaudiologia e Sua Inserção Na Saúde PúblicaDocumento4 pagineA Fonoaudiologia e Sua Inserção Na Saúde PúblicaKyvia Fernanda Tenório100% (1)
- Respira Cao OralDocumento14 pagineRespira Cao Oralana reginaNessuna valutazione finora
- Anamnese GeralDocumento5 pagineAnamnese GeralFgo Wallace SouzaNessuna valutazione finora
- Grupo Consonantal LDocumento3 pagineGrupo Consonantal LDanielle Fraguito100% (1)
- 2 Teste Da Linguinha - MICHELE FONODocumento26 pagine2 Teste Da Linguinha - MICHELE FONOKelly Araújo100% (1)
- MacArthur - ClaudiaSilvaDocumento13 pagineMacArthur - ClaudiaSilvaIngrid RafaellaNessuna valutazione finora
- Lista de Materiais para Motricidade OrofacialDocumento2 pagineLista de Materiais para Motricidade OrofacialDayane macielNessuna valutazione finora
- BCPRDocumento2 pagineBCPRSarah FerrazNessuna valutazione finora
- Avaliação Da Motricidade Oro-FacialDocumento4 pagineAvaliação Da Motricidade Oro-FacialPriscila CristinaNessuna valutazione finora
- Verificação Da Eficiência Da AbordagemDocumento9 pagineVerificação Da Eficiência Da AbordagemEric Oliveira de LimaNessuna valutazione finora
- Efetividade Da Fonoterapia e Proposta de Intervenção Breve em Respiradores OraisDocumento15 pagineEfetividade Da Fonoterapia e Proposta de Intervenção Breve em Respiradores OraisJaviera PalmaNessuna valutazione finora
- Camila GuarnieriDocumento141 pagineCamila GuarnieriCarol Coelho100% (1)
- Artigo Exercicio em M.ODocumento11 pagineArtigo Exercicio em M.OThaís Rodrigues MoraesNessuna valutazione finora
- Disturbio de Leitura e EscritaDocumento5 pagineDisturbio de Leitura e EscritaJohnnatham FillipeNessuna valutazione finora
- Maturidade Simbólica, Vocabulário e Desempenho Intelectual No TDLDocumento6 pagineMaturidade Simbólica, Vocabulário e Desempenho Intelectual No TDLEmanuellen MirandaNessuna valutazione finora
- AUTOMATIZAÇÃO DO /R/ COM FRASESDocumento6 pagineAUTOMATIZAÇÃO DO /R/ COM FRASESAyara FeitosaNessuna valutazione finora
- Respiracao Oral 2Documento11 pagineRespiracao Oral 2Larise Oliveira100% (1)
- LAVE Abril 2010Documento3 pagineLAVE Abril 2010jessicaNessuna valutazione finora
- Aula 021669808314Documento14 pagineAula 021669808314Marcyia Guimaraes100% (1)
- Atividades PAC PDFDocumento1 paginaAtividades PAC PDFFABIANA MARIANO GONÇALVESNessuna valutazione finora
- Afasia Progressiva Primaria Nao FluenteDocumento8 pagineAfasia Progressiva Primaria Nao FluenteAngela BatistaNessuna valutazione finora
- Débora Cattoni Livro Sobre Medidas 20-2-06Documento34 pagineDébora Cattoni Livro Sobre Medidas 20-2-06Pilar Barrios CatalánNessuna valutazione finora
- Avaliação Fonoaudiológica Nas Dificuldades AlimentaresDocumento4 pagineAvaliação Fonoaudiológica Nas Dificuldades AlimentaresLiliane TelesNessuna valutazione finora
- Avaliação MoDocumento7 pagineAvaliação Moluanna lennonNessuna valutazione finora
- JaimeDocumento43 pagineJaimemiguevargas100% (2)
- Fono. Educacional RepositórioDocumento51 pagineFono. Educacional Repositórioceliane sousa100% (1)
- Protocolo de Triagem Da FonoaudiologiaDocumento7 pagineProtocolo de Triagem Da FonoaudiologiaBárbara SenaNessuna valutazione finora
- Resumo Aprender A Escrever Jaime Luiz ZorziDocumento2 pagineResumo Aprender A Escrever Jaime Luiz ZorziTalita Dias BezerraNessuna valutazione finora
- AULA 6 Etapas Da Seleção e Adaptação Dos AASI - Pré MoldagemDocumento5 pagineAULA 6 Etapas Da Seleção e Adaptação Dos AASI - Pré MoldagemAlice BragaNessuna valutazione finora
- Avaliação Do Processamento Auditivo Central (PAC)Documento1 paginaAvaliação Do Processamento Auditivo Central (PAC)djacomNessuna valutazione finora
- Atendimento Fonoaudiológico No Pós FonocirurgiaDocumento8 pagineAtendimento Fonoaudiológico No Pós FonocirurgiafoucaultuffNessuna valutazione finora
- DisartriaDocumento13 pagineDisartriasauloNessuna valutazione finora
- A Mastigação em Pacientes Portadores de Paralisia CerebralDocumento28 pagineA Mastigação em Pacientes Portadores de Paralisia CerebralJulien Bacelar OficialNessuna valutazione finora
- Protocolo DisfagiaDocumento5 pagineProtocolo DisfagiaPriscila Bruno ZancanNessuna valutazione finora
- Gubiani, Marielda BarichelloDocumento146 pagineGubiani, Marielda BarichelloEvaldo CostaNessuna valutazione finora
- Apresentacao Mariangela Stampa WAKDocumento51 pagineApresentacao Mariangela Stampa WAKJoão Oliveira100% (2)
- Estimulação para o Desenvolvimento Da FalaDocumento9 pagineEstimulação para o Desenvolvimento Da FalaRuy Câmara CâmaraNessuna valutazione finora
- Introfono 2Documento5 pagineIntrofono 2vfontanelaNessuna valutazione finora
- Resumo A Voz Do EspecialDocumento5 pagineResumo A Voz Do EspecialVítor Scarpari CitadinNessuna valutazione finora
- Residencia Multiprofissional 2020 - Caderno de Prova - Prog. FonoaudiologiaDocumento14 pagineResidencia Multiprofissional 2020 - Caderno de Prova - Prog. FonoaudiologiaAndréa GarciaNessuna valutazione finora
- O Papel Da EscolaDocumento234 pagineO Papel Da EscolaLuciene MariaNessuna valutazione finora
- Aoerica Moschen RodriguesDocumento12 pagineAoerica Moschen RodriguesAndréa GarciaNessuna valutazione finora
- O Papel Da Escola Na Sociedade ActualDocumento7 pagineO Papel Da Escola Na Sociedade ActualErique BomfimNessuna valutazione finora
- História Da Educação BrasileiraDocumento16 pagineHistória Da Educação BrasileiragutomqNessuna valutazione finora
- O Papel Da Escola Na Sociedade Contemporânea Desafios e PossibilidadesDocumento12 pagineO Papel Da Escola Na Sociedade Contemporânea Desafios e PossibilidadesAndréa GarciaNessuna valutazione finora
- Prova Multi - Fonoaudiologia - PSD 2018Documento12 pagineProva Multi - Fonoaudiologia - PSD 2018Natalia Alustau100% (1)
- ParenteDocumento32 pagineParenteAndréa GarciaNessuna valutazione finora
- A Função Da Escola Na Sociedade ContemporâneaDocumento16 pagineA Função Da Escola Na Sociedade ContemporâneaAndréa GarciaNessuna valutazione finora
- BARROSO-O Estado, A Educacao e A Regulacao Das Politicas PublicasDocumento27 pagineBARROSO-O Estado, A Educacao e A Regulacao Das Politicas PublicasrabelloemailNessuna valutazione finora
- Ceceio AnteriorDocumento7 pagineCeceio AnteriorAndréa GarciaNessuna valutazione finora
- Escola, Conhecimento e Formação de Pessoas - Considerações HistóricasDocumento16 pagineEscola, Conhecimento e Formação de Pessoas - Considerações HistóricasBeatrizJacintodeAlmeidaNessuna valutazione finora
- Ebook Disfagia e Cognicao Paola Pucci Volume 1 1Documento45 pagineEbook Disfagia e Cognicao Paola Pucci Volume 1 1Andréa GarciaNessuna valutazione finora
- É Com OU ?: - ATO - AlinhaDocumento2 pagineÉ Com OU ?: - ATO - AlinhaN MENDESNessuna valutazione finora
- Av de Disfagia Pós ExtubaçãoDocumento9 pagineAv de Disfagia Pós ExtubaçãoAndréa GarciaNessuna valutazione finora
- 06 - Fisiologia RespiratóriaDocumento12 pagine06 - Fisiologia RespiratóriaDany JunqueiraNessuna valutazione finora
- LeituraDocumento4 pagineLeituraAndréa GarciaNessuna valutazione finora
- Anatomia e Fisiologia Do Aparelho Resp Do RNDocumento4 pagineAnatomia e Fisiologia Do Aparelho Resp Do RNAndréa GarciaNessuna valutazione finora
- Aula 12 - Doencas Do Sistema RespiratorioDocumento30 pagineAula 12 - Doencas Do Sistema RespiratorioDaniela DinizNessuna valutazione finora
- Ausculta PulmonarDocumento1 paginaAusculta PulmonarAndréa GarciaNessuna valutazione finora
- 03 - Semiologia Do Aparelho Respiratório Aplicada PDFDocumento22 pagine03 - Semiologia Do Aparelho Respiratório Aplicada PDFLeticia Nogueira100% (1)
- NeurocienciaDocumento73 pagineNeurocienciaTihbello100% (2)
- GabaritoDocumento5 pagineGabaritoAndréa GarciaNessuna valutazione finora
- 05 - Aula 2 TV 08.07 - LP - Prof. AndressaDocumento14 pagine05 - Aula 2 TV 08.07 - LP - Prof. AndressaProf. WirtonNessuna valutazione finora
- Manual Do Acadêmico Estudo DirigidoDocumento2 pagineManual Do Acadêmico Estudo DirigidoElvis JoséNessuna valutazione finora
- 3 Verifificação Da Aprendizagem de Matemática 6º Ano ManhãDocumento6 pagine3 Verifificação Da Aprendizagem de Matemática 6º Ano ManhãEleonilton LeonardoNessuna valutazione finora
- APRESENTAÇÃO Da Alínea A) Apoio Pedagógico PersonalizadoDocumento2 pagineAPRESENTAÇÃO Da Alínea A) Apoio Pedagógico PersonalizadomjrfigueirasNessuna valutazione finora
- Capítulo Vii - Estratégias Metodológicas PDFDocumento100 pagineCapítulo Vii - Estratégias Metodológicas PDFJanice FloraNessuna valutazione finora
- Transferencia 2024 ManualDocumento21 pagineTransferencia 2024 Manualrafaela duarteNessuna valutazione finora
- 150 Frases PsicanáliseDocumento160 pagine150 Frases PsicanáliseAlexandre Falcão Sanseverino100% (2)
- Contatos UFT ReitoriaeCâmpus (GeralConsolidado)Documento26 pagineContatos UFT ReitoriaeCâmpus (GeralConsolidado)Adriana PinheiroNessuna valutazione finora
- Organizacao Das Sessoes de Coaching PDFDocumento2 pagineOrganizacao Das Sessoes de Coaching PDFViviane Alves100% (3)
- Resumo Teorias Da PersonalidadeDocumento14 pagineResumo Teorias Da PersonalidadePhillarts Lopes50% (2)
- Relatório Pós-Doutorado FEUSP - Paulo C. A. RaboniDocumento59 pagineRelatório Pós-Doutorado FEUSP - Paulo C. A. RaboniPaulo C A RaboniNessuna valutazione finora
- Desenvolvimento e Aprendizagem MotoraDocumento23 pagineDesenvolvimento e Aprendizagem MotoraFrancilene VieiraNessuna valutazione finora
- Seduccod 03 Gab 1Documento18 pagineSeduccod 03 Gab 1Rebeca AngelimNessuna valutazione finora
- Análise de Relato HistóricoDocumento25 pagineAnálise de Relato HistóricocatarinapiresNessuna valutazione finora
- Monitores Campos de Férias (Curso de Évora) - Ficha de InscriçãoDocumento2 pagineMonitores Campos de Férias (Curso de Évora) - Ficha de Inscriçãopussinbuts100% (2)
- Texto 01 A Descoberta Da InfânciaDocumento13 pagineTexto 01 A Descoberta Da InfânciaAnonymous rMYPpUA1100% (1)
- ndo2S1icm0ZoMiKCNRkDedson Carli Aula 01Documento81 paginendo2S1icm0ZoMiKCNRkDedson Carli Aula 01Juliana GonçalvesNessuna valutazione finora
- Apostila 1 Fevereiro 8anoDocumento14 pagineApostila 1 Fevereiro 8anotarcisioNessuna valutazione finora
- Dissertação Marcos Santos PDFDocumento171 pagineDissertação Marcos Santos PDFDuda OliveNessuna valutazione finora
- Trampolim - Língua PortuguesaDocumento144 pagineTrampolim - Língua PortuguesaFilipa EstrelaNessuna valutazione finora
- Portfolio NicmaDocumento10 paginePortfolio NicmaMaurício Rodrigues FredericoNessuna valutazione finora
- ActaDocumento13 pagineActaReis DanilsaNessuna valutazione finora
- ++plano de Curso e Unidade - Divulgando Com Jesus - Revisar As PráticasDocumento76 pagine++plano de Curso e Unidade - Divulgando Com Jesus - Revisar As Práticasmarcia_laerce3404Nessuna valutazione finora
- 1° Simulado AFADocumento26 pagine1° Simulado AFARECRUTA COUTONessuna valutazione finora
- Plano de Aula para Educação Infantil IDocumento12 paginePlano de Aula para Educação Infantil IMichelle Caldas67% (3)