Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- CASSEEEDocumento6 pagineCASSEEEBen Paolo Cecilia RabaraNessuna valutazione finora
- Salient Features of The PatientDocumento2 pagineSalient Features of The PatientBen Paolo Cecilia RabaraNessuna valutazione finora
- 4 Day RoutineDocumento310 pagine4 Day RoutineBen Paolo Cecilia Rabara0% (1)
- Training Program For HypertrophyDocumento217 pagineTraining Program For HypertrophyBen Paolo Cecilia RabaraNessuna valutazione finora
- 60 in 60Documento10 pagine60 in 60Ben Paolo Cecilia RabaraNessuna valutazione finora
- Erythematous Lesions PDF-notes 201610271601Documento17 pagineErythematous Lesions PDF-notes 201610271601Ben Paolo Cecilia RabaraNessuna valutazione finora
- Iron Buff 22052019Documento201 pagineIron Buff 22052019Ben Paolo Cecilia RabaraNessuna valutazione finora
- CASSEEEDocumento6 pagineCASSEEEBen Paolo Cecilia RabaraNessuna valutazione finora
- Diaz V People and Levi Strauss (2013) : FactsDocumento1 paginaDiaz V People and Levi Strauss (2013) : FactsDiane AngelineNessuna valutazione finora
- Erythematous Lesions PDF-notes 201610271601Documento17 pagineErythematous Lesions PDF-notes 201610271601Ben Paolo Cecilia RabaraNessuna valutazione finora
- PGI Graduation 2019 FinalDocumento153 paginePGI Graduation 2019 FinalBen Paolo Cecilia RabaraNessuna valutazione finora
- Book OneDocumento15 pagineBook OneBen Paolo Cecilia RabaraNessuna valutazione finora
- Pediatric CalculatorDocumento3 paginePediatric CalculatorBen Paolo Cecilia RabaraNessuna valutazione finora
- Guide To Adulting 101 by Paps MDDocumento2 pagineGuide To Adulting 101 by Paps MDBen Paolo Cecilia Rabara0% (1)
- Neonatal HypoglycemiaDocumento11 pagineNeonatal HypoglycemiaBen Paolo Cecilia Rabara100% (1)
- Peds0813 Motor Vehicle TraumaDocumento28 paginePeds0813 Motor Vehicle TraumaBen Paolo Cecilia RabaraNessuna valutazione finora
- Ice Cream FitnessDocumento54 pagineIce Cream FitnessBen Paolo Cecilia RabaraNessuna valutazione finora
- SEO Fast Start:: A Simple, Step by Step System For Better ResultsDocumento117 pagineSEO Fast Start:: A Simple, Step by Step System For Better ResultsNeven ErkićNessuna valutazione finora
- Boehringer Ingelheim Leadership RolesDocumento1 paginaBoehringer Ingelheim Leadership RolesBen Paolo Cecilia RabaraNessuna valutazione finora
- 2MEDICINE8 Thyroid Gland Disorders UERM2015B PDFDocumento16 pagine2MEDICINE8 Thyroid Gland Disorders UERM2015B PDFBen Paolo Cecilia Rabara100% (1)
- Summary of Encyclical LettersDocumento4 pagineSummary of Encyclical LettersBen Paolo Cecilia RabaraNessuna valutazione finora
- Drug Info Inquiry FormDocumento1 paginaDrug Info Inquiry FormBen Paolo Cecilia RabaraNessuna valutazione finora
- Pharmaceutical Incompatibilities GuideDocumento7 paginePharmaceutical Incompatibilities GuideBen Paolo Cecilia Rabara88% (8)
- 3 IdiotsDocumento1 pagina3 IdiotsBen Paolo Cecilia RabaraNessuna valutazione finora
- SAR of Macrolides, Penicillins, and Other AntibioticsDocumento36 pagineSAR of Macrolides, Penicillins, and Other AntibioticsBen Paolo Cecilia RabaraNessuna valutazione finora
- National Children's HospitalDocumento9 pagineNational Children's HospitalBen Paolo Cecilia RabaraNessuna valutazione finora
- Alkajohn LoidDocumento9 pagineAlkajohn LoidBen Paolo Cecilia RabaraNessuna valutazione finora
- pH Measurement and Buffer Preparation GuideDocumento3 paginepH Measurement and Buffer Preparation GuideBen Paolo Cecilia Rabara100% (2)
- Ben Paolo CDocumento1 paginaBen Paolo CBen Paolo Cecilia RabaraNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
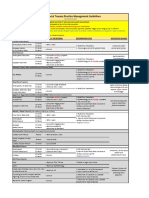
- VUMC Facial Trauma Practice Management GuidelinesDocumento1 paginaVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNessuna valutazione finora
- The Difficult or Failed Airway: Pat Melanson, MDDocumento28 pagineThe Difficult or Failed Airway: Pat Melanson, MDMinorC3Nessuna valutazione finora
- Cranial Nerves Assessment GuideDocumento8 pagineCranial Nerves Assessment GuideTrisha Najial AlmendraNessuna valutazione finora
- Surface Anatomy: David Ebenezer Department of Anatomy Velammal Medical CollegeDocumento101 pagineSurface Anatomy: David Ebenezer Department of Anatomy Velammal Medical CollegeKarishma RameshNessuna valutazione finora
- Board Review Questions EmergencyDocumento331 pagineBoard Review Questions Emergencyمعتز حرارة100% (1)
- Frog Dissection GuideDocumento9 pagineFrog Dissection GuideEloisa Baquista BatengaNessuna valutazione finora
- Vein Vs ArteryDocumento4 pagineVein Vs ArterySaarwin MuruganNessuna valutazione finora
- Introduction to Autonomic PharmacologyDocumento30 pagineIntroduction to Autonomic PharmacologyImrana AamirNessuna valutazione finora
- The Wrist ComplexDocumento35 pagineThe Wrist ComplexKeshav Singhmaar AryaNessuna valutazione finora
- English-Italian Medical TermsDocumento12 pagineEnglish-Italian Medical Termsionicaa3Nessuna valutazione finora
- Muscular SystemDocumento41 pagineMuscular SystemGem Rose UretaNessuna valutazione finora
- Boala Polichistica Hepato-RenalaDocumento1 paginaBoala Polichistica Hepato-RenaladoinaNessuna valutazione finora
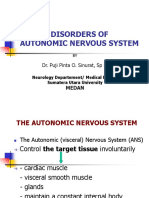
- K5 - Disorders of Autonomic Nervous SystemDocumento47 pagineK5 - Disorders of Autonomic Nervous Systemengkiii100% (1)
- Blood Vessels and Circulation 1Documento36 pagineBlood Vessels and Circulation 1Kuya RnJNessuna valutazione finora
- Breathing For Singing-The Anatomy of RespirationDocumento11 pagineBreathing For Singing-The Anatomy of RespirationAnurrag Kumar100% (3)
- Changes To Breast Structure and Function Across ADocumento12 pagineChanges To Breast Structure and Function Across AMauricio MoncadaNessuna valutazione finora
- MobilizationDocumento15 pagineMobilizationGladwin MahibanNessuna valutazione finora
- Fines DirumahDocumento33 pagineFines DirumahJohn Atox PetrucciNessuna valutazione finora
- Anatomy of Spinal Cord and Spinal Nerves, Reflexes, and Reaction Time and LearningDocumento32 pagineAnatomy of Spinal Cord and Spinal Nerves, Reflexes, and Reaction Time and LearningMickeyNessuna valutazione finora
- Too Cold Too TiredDocumento66 pagineToo Cold Too TiredPatricia Lawler75% (4)
- Sullivan Siegelman Retention Exam With AnswersDocumento9 pagineSullivan Siegelman Retention Exam With AnswersJed A. MartirNessuna valutazione finora
- The Contents of Anatomical Snuff Box AreDocumento3 pagineThe Contents of Anatomical Snuff Box AreZimam ZamriNessuna valutazione finora
- Welcome To Month 24 of Booty by Bret!: This Month Is A & PlanDocumento12 pagineWelcome To Month 24 of Booty by Bret!: This Month Is A & PlanGeraldyne100% (2)
- Discussion Notes (Anaphy)Documento49 pagineDiscussion Notes (Anaphy)jade tanNessuna valutazione finora
- Dental Morphology - An Illustrated Guide - Beek, Geoffrey C. Van - 1983 - Bristol Boston - Wright-PSG - 9780723606666 - Anna's ArchiveDocumento148 pagineDental Morphology - An Illustrated Guide - Beek, Geoffrey C. Van - 1983 - Bristol Boston - Wright-PSG - 9780723606666 - Anna's Archivedb nklttNessuna valutazione finora
- Non Operative Proximal Humeral FXDocumento2 pagineNon Operative Proximal Humeral FXAdmirNessuna valutazione finora
- Physical Fitness GuideDocumento9 paginePhysical Fitness GuidePaulyn Jhoy FajardoNessuna valutazione finora
- Senses and their Functions Explained in 40 CharactersDocumento34 pagineSenses and their Functions Explained in 40 CharactersAce Vincent LunaNessuna valutazione finora
- Anatomy of the Lumbar SpineDocumento39 pagineAnatomy of the Lumbar Spinepasha100% (1)
- 3-Cervical RadiculopathyDocumento7 pagine3-Cervical RadiculopathyAmimul EhsanNessuna valutazione finora