Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Recavery After Anasthesia PDFDocumento3 pagineRecavery After Anasthesia PDFYudionoNessuna valutazione finora
- Neurovascular Assesment PDFDocumento9 pagineNeurovascular Assesment PDFYudionoNessuna valutazione finora
- Prevention of Tourniquet Paralysis PDFDocumento5 paginePrevention of Tourniquet Paralysis PDFYudionoNessuna valutazione finora
- Respiratory Failure (Aan) PDFDocumento19 pagineRespiratory Failure (Aan) PDFYudionoNessuna valutazione finora
- Respiratory Failure (Aan) PDFDocumento19 pagineRespiratory Failure (Aan) PDFYudionoNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Drugs Acting On CNS: Prof. A O Elkhawad Umst Khartoum, SudanDocumento80 pagineDrugs Acting On CNS: Prof. A O Elkhawad Umst Khartoum, SudanmekaielNessuna valutazione finora
- Practice Questions - EDNDocumento6 paginePractice Questions - EDNKaren BlancoNessuna valutazione finora
- Medicine Lecture One General Anaethsia 19th NovDocumento102 pagineMedicine Lecture One General Anaethsia 19th NovIrene Zae MwandotoNessuna valutazione finora
- Rectal Sedation: Chapter OutlineDocumento5 pagineRectal Sedation: Chapter OutlinepoonpatchaNessuna valutazione finora
- LEARNING MODULE IN NCM 106 Final Peroid 2Documento30 pagineLEARNING MODULE IN NCM 106 Final Peroid 2Threcia RotaNessuna valutazione finora
- Anesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFDocumento125 pagineAnesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFKatarina SimicicNessuna valutazione finora
- Guymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaDocumento93 pagineGuymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaKe Xu100% (1)
- Delirium in The Elderly: by Sue Fosnight, Bspharm, BCPS, CGPDocumento24 pagineDelirium in The Elderly: by Sue Fosnight, Bspharm, BCPS, CGPChika SabaNessuna valutazione finora
- Assessment and Treatment of The WithdrawalDocumento13 pagineAssessment and Treatment of The Withdrawalfuka priesleyNessuna valutazione finora
- Effects of Electroacupuncture in A Mouse Model of Experimentally-Induced OsteosarcomaDocumento196 pagineEffects of Electroacupuncture in A Mouse Model of Experimentally-Induced Osteosarcomabebe_roalbaNessuna valutazione finora
- ClinicalOpiateWithdrawalScale PDFDocumento2 pagineClinicalOpiateWithdrawalScale PDFRajamanitiNessuna valutazione finora
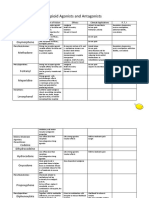
- Opioid Agonists and AntagonistsDocumento5 pagineOpioid Agonists and AntagonistsCas BuNessuna valutazione finora
- NG163Documento24 pagineNG163Tim BrownNessuna valutazione finora
- Pediatric Pain Management: Avni M. Bhalakia M.D. St. Barnabas HospitalDocumento57 paginePediatric Pain Management: Avni M. Bhalakia M.D. St. Barnabas HospitalNurul HasanNessuna valutazione finora
- Addiction A Very Short Introduction Keith Humphreys Full ChapterDocumento67 pagineAddiction A Very Short Introduction Keith Humphreys Full Chapterjustin.martin277100% (3)
- Device Related Error in Patient Controlled.17Documento6 pagineDevice Related Error in Patient Controlled.17Ali ÖzdemirNessuna valutazione finora
- RAPIFEN AlfentanilDocumento5 pagineRAPIFEN AlfentanilivankostadinovNessuna valutazione finora
- Sedation and Analgesia in ICU FinalDocumento68 pagineSedation and Analgesia in ICU FinalAsim KhanNessuna valutazione finora
- Concept Map For EndocarditisDocumento3 pagineConcept Map For EndocarditisSavanna ChambersNessuna valutazione finora
- IV PCDocumento27 pagineIV PCNusrat Jahan MuniaNessuna valutazione finora
- Drug Study On Emergency DrugsDocumento16 pagineDrug Study On Emergency DrugsJosepNessuna valutazione finora
- Oral Drug Delivery 07Documento28 pagineOral Drug Delivery 07Yuppie RajNessuna valutazione finora
- WalshcDocumento26 pagineWalshcapi-530445129Nessuna valutazione finora
- "Is There A Doctor On Board - " The Plight of The In-Flight Orthopaedic SurgeonDocumento8 pagine"Is There A Doctor On Board - " The Plight of The In-Flight Orthopaedic SurgeonRajiv TanwarNessuna valutazione finora
- Maximizing Pain Management in Cancer Patients - DR Ungku KamariahDocumento36 pagineMaximizing Pain Management in Cancer Patients - DR Ungku Kamariahmalaysianhospicecouncil6240Nessuna valutazione finora
- Abstracts of The 2018 AANS/CNS Joint Section On Disorders of The Spine and Peripheral Nerves Annual MeetingDocumento109 pagineAbstracts of The 2018 AANS/CNS Joint Section On Disorders of The Spine and Peripheral Nerves Annual MeetingEka Wahyu HerdiyantiNessuna valutazione finora
- Comfort and Pain ManagementDocumento75 pagineComfort and Pain ManagementBeverly Lavilla100% (1)
- Ketamine 1Documento20 pagineKetamine 1fadil23Nessuna valutazione finora
- Ipi Nursing Part 1,2,3Documento53 pagineIpi Nursing Part 1,2,3Noleen MckayNessuna valutazione finora
- National Pain ManagementDocumento86 pagineNational Pain ManagementabelNessuna valutazione finora