Potrebbero piacerti anche
- BlepharoplastyDocumento23 pagineBlepharoplastyNur baitiNessuna valutazione finora
- Y3 T2 PAM CWU 2 - Acute BronchiolitisDocumento7 pagineY3 T2 PAM CWU 2 - Acute Bronchiolitisanon_67984147Nessuna valutazione finora
- Long Case Surgery Exam QuestionDocumento25 pagineLong Case Surgery Exam Questionwhee182Nessuna valutazione finora
- Farah Cwu Obstetric EditDocumento19 pagineFarah Cwu Obstetric EditfarahNessuna valutazione finora
- EM Case Write UpDocumento11 pagineEM Case Write UpRaihana Rafi100% (2)
- CWU MedicineDocumento37 pagineCWU MedicineAzizi Abd RahmanNessuna valutazione finora
- OSCE Qs Internal MedicineDocumento29 pagineOSCE Qs Internal MedicineRancesh Famo0% (1)
- O&G Long Case Exam QuestionDocumento21 pagineO&G Long Case Exam Questionwhee182Nessuna valutazione finora
- Pharmacotherapy of ArrythmiasDocumento68 paginePharmacotherapy of ArrythmiasABREHAM BUKULONessuna valutazione finora
- USMLE High Yield Internal Medicine Notes-Part I 2020Documento19 pagineUSMLE High Yield Internal Medicine Notes-Part I 2020usmlematerials.netNessuna valutazione finora
- Pediatric Clinical ExaminationDocumento3 paginePediatric Clinical ExaminationAlexander EnnesNessuna valutazione finora
- Case Write Up 1-CholecystitisDocumento9 pagineCase Write Up 1-CholecystitisAmbhi Gana100% (1)
- Hernia Examination SchemeDocumento4 pagineHernia Examination Schemeatribecalledquest20Nessuna valutazione finora
- CWU 2 - Complicated PneumoniaDocumento44 pagineCWU 2 - Complicated PneumoniaJared Khoo Er Hau100% (1)
- Cwu Ortho TraumaDocumento9 pagineCwu Ortho TraumaMia MusNessuna valutazione finora
- Upper GIT BleedingDocumento69 pagineUpper GIT BleedingSoleh Ramly100% (1)
- Case Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorDocumento21 pagineCase Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorwhosenahNessuna valutazione finora
- Powerpoint: Disorders of The Thyroid GlandDocumento67 paginePowerpoint: Disorders of The Thyroid Glandj.doe.hex_87100% (1)
- UMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiDocumento132 pagineUMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiUchiha AnzarNessuna valutazione finora
- CWU 1 SurgeryDocumento23 pagineCWU 1 SurgeryAmelia AkmarNessuna valutazione finora
- CWU OrthopedicsDocumento6 pagineCWU OrthopedicsSana Anam JahanNessuna valutazione finora
- Case Write Up-DengueDocumento16 pagineCase Write Up-DengueSyafi'ie Syukri100% (1)
- Surgery Long Case - Cholecystitis ObstructiveDocumento33 pagineSurgery Long Case - Cholecystitis Obstructivegplabon100% (2)
- Cwu Surgery Y5 AsyikinDocumento21 pagineCwu Surgery Y5 AsyikinNurulasyikin MAANessuna valutazione finora
- Case Write Up 2Documento16 pagineCase Write Up 2Shidev100% (1)
- Cwu Ong TwinDocumento14 pagineCwu Ong TwinAiman ArifinNessuna valutazione finora
- Waiver For Blood DonationDocumento4 pagineWaiver For Blood Donationeleazar_magsino08Nessuna valutazione finora
- Pediatrics CWU Year 5Documento7 paginePediatrics CWU Year 5anon_67984147Nessuna valutazione finora
- Thyroid Gland OSCE ExaminationDocumento13 pagineThyroid Gland OSCE ExaminationkylieverNessuna valutazione finora
- Explanation LetterDocumento1 paginaExplanation LettersaufisafingiNessuna valutazione finora
- Genetics Practice NCLEX Questions HandoutDocumento6 pagineGenetics Practice NCLEX Questions HandoutAlvin L. Rozier100% (3)
- Acute Appendicitis: Surgical PostingDocumento8 pagineAcute Appendicitis: Surgical PostingGraldoNessuna valutazione finora
- Case Write Up SurgeryDocumento13 pagineCase Write Up SurgerySharvin100% (3)
- DRUG STUDY: Fenofibrate - TricorDocumento2 pagineDRUG STUDY: Fenofibrate - TricorYum CNessuna valutazione finora
- Mitral Valve ProlapseDocumento7 pagineMitral Valve ProlapsehracakNessuna valutazione finora
- StomasDocumento4 pagineStomasSaravanan Sridharan100% (1)
- Medicine Long CaseDocumento26 pagineMedicine Long Casewhee182Nessuna valutazione finora
- Write Up Surgery 1 TambahDocumento22 pagineWrite Up Surgery 1 Tambahazizi abd rahmanNessuna valutazione finora
- Bronchial AsthmaDocumento54 pagineBronchial AsthmaSehar162100% (2)
- DermaDocumento30 pagineDermalydia_chandraNessuna valutazione finora
- Nursing Diagnosis and Nursing Interventions For Dengue Hemorrhagic FeverDocumento2 pagineNursing Diagnosis and Nursing Interventions For Dengue Hemorrhagic FeverThirdy Aquino82% (28)
- Breast CarcinomaDocumento13 pagineBreast Carcinomamegat120288100% (1)
- NCP Proper CholecystectomyDocumento2 pagineNCP Proper CholecystectomyGail Lian SantosNessuna valutazione finora
- Clerking An o & G CaseDocumento57 pagineClerking An o & G CaseAlan Na100% (2)
- Cwu - SurgeryDocumento10 pagineCwu - SurgeryThiviyaa SivaselvamNessuna valutazione finora
- Name: Wong Wai Kheong Matrix No: BMS12081154Documento13 pagineName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNessuna valutazione finora
- Case Write UpDocumento9 pagineCase Write UpAsraf LatifNessuna valutazione finora
- Case Write Up Harmeet Multinodular GoitreDocumento29 pagineCase Write Up Harmeet Multinodular GoitreDevikha PeremelNessuna valutazione finora
- Anaest CWU OTDocumento15 pagineAnaest CWU OTHana Fauzi100% (1)
- Derma Case Write UpDocumento9 pagineDerma Case Write UpAmbhi GanaNessuna valutazione finora
- CPC Acute AppendicitisDocumento57 pagineCPC Acute AppendicitisYS Nate100% (1)
- Acute AbdomenDocumento24 pagineAcute AbdomenGrace SimmonsNessuna valutazione finora
- Thyroid Neoplasms: Kelompok 3 Dr. Reza Maulana Dr. Intan E. Napitupulu Drg. Andi Arfandi ArifuddinDocumento41 pagineThyroid Neoplasms: Kelompok 3 Dr. Reza Maulana Dr. Intan E. Napitupulu Drg. Andi Arfandi ArifuddinIntan Eklesiana NapitupuluNessuna valutazione finora
- Surgery Case WriteDocumento2 pagineSurgery Case WriteDat PhamNessuna valutazione finora
- Cwu Breast AbscessDocumento10 pagineCwu Breast AbscessfarahmazlanNessuna valutazione finora
- GDD ? H@Qka A9Fk KMJ? GFK H9Cakl9F: Clinical & Toacs Fcps Examination PaediatricsDocumento3 pagineGDD ? H@Qka A9Fk KMJ? GFK H9Cakl9F: Clinical & Toacs Fcps Examination PaediatricsBabarNaeemNessuna valutazione finora
- Shivaani (Internal Medicine CWU)Documento12 pagineShivaani (Internal Medicine CWU)S.M. Manogaran Shivaani AP S.M. ManogaranNessuna valutazione finora
- Fistula in AnoDocumento27 pagineFistula in AnoRaissa Pauline Oliva0% (1)
- A. Brief Definition of The Specific Disease Condition: Mechanism CauseDocumento6 pagineA. Brief Definition of The Specific Disease Condition: Mechanism CauseEuniceNessuna valutazione finora
- Pre Exam Surgical Notes 2Documento166 paginePre Exam Surgical Notes 2flor vickyNessuna valutazione finora
- Examination of A StomaDocumento3 pagineExamination of A StomaChloe100% (1)
- CFCSDocumento77 pagineCFCSNurul NadiahNessuna valutazione finora
- 20 - Toronto Notes 2011 - Ophthamology PDFDocumento46 pagine20 - Toronto Notes 2011 - Ophthamology PDFSisterzzShopDua0% (1)
- Case Write Up FibroidDocumento17 pagineCase Write Up FibroidNadsri AmirNessuna valutazione finora
- Isotonic Saline (0.9%Nacl-Normal Saline) IndicationDocumento3 pagineIsotonic Saline (0.9%Nacl-Normal Saline) IndicationJared AllenNessuna valutazione finora
- Haemorrhoid-Clinical Case Discussion 2Documento15 pagineHaemorrhoid-Clinical Case Discussion 2jong siangNessuna valutazione finora
- R 8Documento9 pagineR 8Sadia AwanNessuna valutazione finora
- Surgery 1 Clinical Case Discussion: School of MedicineDocumento20 pagineSurgery 1 Clinical Case Discussion: School of MedicineJong SiangNessuna valutazione finora
- ObGyn CWU 3Documento16 pagineObGyn CWU 3ppmmttkkccNessuna valutazione finora
- List Products RM10Documento6 pagineList Products RM10AthirahRaraNessuna valutazione finora
- Must Know Common Drugs For HODocumento6 pagineMust Know Common Drugs For HOAthirahRaraNessuna valutazione finora
- 11mastering Medical Long CaseDocumento42 pagine11mastering Medical Long CaseAthirahRaraNessuna valutazione finora
- CSKL 1b - Mechanism of LabourDocumento19 pagineCSKL 1b - Mechanism of LabourAthirahRara100% (1)
- Tips ProDocumento1 paginaTips ProAthirahRaraNessuna valutazione finora
- OBG Prep HODocumento4 pagineOBG Prep HOAthirahRaraNessuna valutazione finora
- Bom Bala Ka Bombalaka AyyDocumento1 paginaBom Bala Ka Bombalaka AyyAthirahRaraNessuna valutazione finora
- Letter of Consent Baru PDFDocumento1 paginaLetter of Consent Baru PDFAthirahRaraNessuna valutazione finora
- Medical Based Long Cases Internal Medicine Paediatrics April 2019Documento4 pagineMedical Based Long Cases Internal Medicine Paediatrics April 2019AthirahRaraNessuna valutazione finora
- Bom Bala Ka Bombalaka AyyDocumento1 paginaBom Bala Ka Bombalaka AyyAthirahRaraNessuna valutazione finora
- Syphilis Can Be Staged Into PrimaryDocumento2 pagineSyphilis Can Be Staged Into PrimaryAthirahRaraNessuna valutazione finora
- Tugasan HarianDocumento1 paginaTugasan HarianAthirahRaraNessuna valutazione finora
- DR Subha OspeDocumento3 pagineDR Subha OspeAthirahRaraNessuna valutazione finora
- Room ArrangementDocumento3 pagineRoom ArrangementAthirahRaraNessuna valutazione finora
- Ka and KB ConstantDocumento1 paginaKa and KB ConstantAthirahRaraNessuna valutazione finora
- Anemia NoteDocumento1 paginaAnemia NoteAthirahRaraNessuna valutazione finora
- Glo Me Rulo NephritisDocumento21 pagineGlo Me Rulo NephritisAthirahRara100% (1)
- 1Documento1 pagina1AthirahRaraNessuna valutazione finora
- Polycystic Kidney Disease: 1. Autosomal Recessive 2.autosomal DominantDocumento20 paginePolycystic Kidney Disease: 1. Autosomal Recessive 2.autosomal DominantAthirahRaraNessuna valutazione finora
- Quadratic EquationsDocumento2 pagineQuadratic EquationsAthirahRaraNessuna valutazione finora
- Discussion GeneticDocumento10 pagineDiscussion GeneticAthirahRaraNessuna valutazione finora
- Pathophysiology of Chronic Renal Failure PDFDocumento4 paginePathophysiology of Chronic Renal Failure PDFDewa Made Rendy SanjayaNessuna valutazione finora
- 1 Staphylococcus Lecture 1 Last YearDocumento39 pagine1 Staphylococcus Lecture 1 Last YearKeshant Samaroo100% (1)
- ENDOMETRIOSISDocumento33 pagineENDOMETRIOSISpriyanka bhowmikNessuna valutazione finora
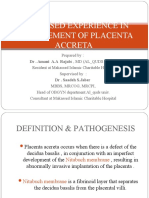
- Makassed Experience in Management of Placenta AccretaDocumento39 pagineMakassed Experience in Management of Placenta AccretaRaluca HabaNessuna valutazione finora
- XXXXXX 121Documento11 pagineXXXXXX 121AndriantkNessuna valutazione finora
- Posterior Uveitis HandoutDocumento4 paginePosterior Uveitis Handoutdanny wiryaNessuna valutazione finora
- Modul Semester 1-1Documento44 pagineModul Semester 1-1yuriNessuna valutazione finora
- Role of LABACS Provides A Simple and Effective For COPD and Asthma ManagementDocumento74 pagineRole of LABACS Provides A Simple and Effective For COPD and Asthma ManagementHans WinardiNessuna valutazione finora
- Jama Echouffotcheugui 2023 RV 230007 1680895578.04302Documento11 pagineJama Echouffotcheugui 2023 RV 230007 1680895578.04302Buton InspirasiNessuna valutazione finora
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Test Name ResultDocumento3 pagineD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Test Name ResultShaikh EsaNessuna valutazione finora
- Case Presentation SiliconomaDocumento24 pagineCase Presentation Siliconomaentgo8282Nessuna valutazione finora
- The Nurse in The Emergency Department Is Caring For A Patient With A PartialDocumento13 pagineThe Nurse in The Emergency Department Is Caring For A Patient With A Partialhasan ahmdNessuna valutazione finora
- Workup For ProteinuriaDocumento17 pagineWorkup For ProteinuriaSantiago ChávezNessuna valutazione finora
- MS Musculoskeletal ReviewDocumento12 pagineMS Musculoskeletal ReviewShayesra-Radina Laja SahibadNessuna valutazione finora
- Pediatrics, Geriatrics and Clinical MicrobiologyDocumento15 paginePediatrics, Geriatrics and Clinical MicrobiologySelvakumardxbNessuna valutazione finora
- Ovarian Cancer: A. IntroductionDocumento10 pagineOvarian Cancer: A. IntroductionBer AnneNessuna valutazione finora
- Biology ProjectDocumento18 pagineBiology Projectladheedha69% (13)
- Benign Gynecologic Lesion of The VulvaDocumento8 pagineBenign Gynecologic Lesion of The VulvaKristine VanzuelaNessuna valutazione finora
- Anionic GapDocumento8 pagineAnionic GapMaria-Larisa HohanNessuna valutazione finora
- Review 02Documento2 pagineReview 02Vicki KimNessuna valutazione finora