Potrebbero piacerti anche
- Letters: Trends in Diagnoses of HIV Infection in The United States, 2002-2011Documento3 pagineLetters: Trends in Diagnoses of HIV Infection in The United States, 2002-2011IietAyu05Nessuna valutazione finora
- EtsDocumento31 pagineEtsTony Gomez Luna LeyvaNessuna valutazione finora
- Human Immunodeficiency Virus, Other Sexually Transmitted Infections, and Sexual and Reproductive Health in Lesbian, Gay, Bisexual, Transgender YouthDocumento29 pagineHuman Immunodeficiency Virus, Other Sexually Transmitted Infections, and Sexual and Reproductive Health in Lesbian, Gay, Bisexual, Transgender YouthRoman_1988Nessuna valutazione finora
- Ensuring Access To Sexually Transmitted Infection Care For AllDocumento13 pagineEnsuring Access To Sexually Transmitted Infection Care For AllCenter for American ProgressNessuna valutazione finora
- Among Youth: Hiv/AidsDocumento5 pagineAmong Youth: Hiv/AidsShahnaz RizkaNessuna valutazione finora
- Journal Hiv - Aids: Disusun Untuk Memenuhi Tugas Mata Kuliah Keperawatan HIV-AIDSDocumento13 pagineJournal Hiv - Aids: Disusun Untuk Memenuhi Tugas Mata Kuliah Keperawatan HIV-AIDSarya andika saputraNessuna valutazione finora
- Aspectos Biológicos, Terapeuticos en Mujeres Con VIH Comparado A Hombres AIDS ReviewDocumento8 pagineAspectos Biológicos, Terapeuticos en Mujeres Con VIH Comparado A Hombres AIDS ReviewIsmaelJoséGonzálezGuzmánNessuna valutazione finora
- First Page PDFDocumento1 paginaFirst Page PDFLeidy Constanza Villalobos GonzalezNessuna valutazione finora
- CDC FACT SHEET: Reported STDs in The United States - 2012 National Data For Chlamydia, Gonorrhea, and SyphilisDocumento3 pagineCDC FACT SHEET: Reported STDs in The United States - 2012 National Data For Chlamydia, Gonorrhea, and Syphilistherepubliq.comNessuna valutazione finora
- STD Powerpoint Presentation-2Documento14 pagineSTD Powerpoint Presentation-2api-253644735Nessuna valutazione finora
- Ten Things Gay Men Should Discuss With Their Health Care ProvidersDocumento3 pagineTen Things Gay Men Should Discuss With Their Health Care ProvidersDante SpardaNessuna valutazione finora
- Clinical Update in SexuallyDocumento11 pagineClinical Update in SexuallyAfiqah So JasmiNessuna valutazione finora
- Pi Is 0027968415301292Documento8 paginePi Is 0027968415301292yasahswi91Nessuna valutazione finora
- HIV Among Youth: The NumbersDocumento2 pagineHIV Among Youth: The NumbersJoseph RichardsonNessuna valutazione finora
- Sexuality, Sexual Health, and Sexually Transmitted Infections in Adolescents and Young AdultsDocumento4 pagineSexuality, Sexual Health, and Sexually Transmitted Infections in Adolescents and Young AdultsyehkzprxisluvsstrvNessuna valutazione finora
- NIH Public Access: Author ManuscriptDocumento13 pagineNIH Public Access: Author ManuscriptYeli AstiNessuna valutazione finora
- 1471 2458 13 1122 PDFDocumento9 pagine1471 2458 13 1122 PDFShintia Theresia LumempouwNessuna valutazione finora
- Super Final Output (For Hardbound)Documento108 pagineSuper Final Output (For Hardbound)Melody Kaye MonsantoNessuna valutazione finora
- Body Image Impacts Risky Behavior in Youth with HIVDocumento6 pagineBody Image Impacts Risky Behavior in Youth with HIVMorrison Omokiniovo Jessa SnrNessuna valutazione finora
- STD Screening and PreventionDocumento12 pagineSTD Screening and PreventionjordyeeNessuna valutazione finora
- Understanding Men's Health and Use of Violence: Interface of Rape and HIV in South Africa (2009)Documento2 pagineUnderstanding Men's Health and Use of Violence: Interface of Rape and HIV in South Africa (2009)Children's InstituteNessuna valutazione finora
- Hiv Aids Thesis TopicsDocumento5 pagineHiv Aids Thesis TopicsCollegePapersHelpSingapore100% (1)
- Strategies for Awareness & Prevention of Hiv/Aids Among African-Americans: A Hand BookDa EverandStrategies for Awareness & Prevention of Hiv/Aids Among African-Americans: A Hand BookNessuna valutazione finora
- Product1 1Documento4 pagineProduct1 1api-444918976Nessuna valutazione finora
- Artikel-Hiv-Ayu NingrumDocumento7 pagineArtikel-Hiv-Ayu NingrumAyu NingrumNessuna valutazione finora
- Faktor-Faktor Risiko Penularan Hiv/Aids Pada Laki-Laki Dengan Orientasi Seks Heteroseksual Dan Homoseksual Di PurwokertoDocumento11 pagineFaktor-Faktor Risiko Penularan Hiv/Aids Pada Laki-Laki Dengan Orientasi Seks Heteroseksual Dan Homoseksual Di PurwokertoTriska Valentina RaharjoNessuna valutazione finora
- Sexually Transmitted Diseases Among Adolescents in Developed CountriesDocumento16 pagineSexually Transmitted Diseases Among Adolescents in Developed CountriesJudith AmarteyNessuna valutazione finora
- How HIV Is DetectedDocumento12 pagineHow HIV Is DetectedTaranisaNessuna valutazione finora
- Top 10 forGayMenDocumento1 paginaTop 10 forGayMenBeatriz SantiagoNessuna valutazione finora
- Dutton, Koenig, & Fennie, 2008Documento7 pagineDutton, Koenig, & Fennie, 2008Anonymous 75M6uB3OwNessuna valutazione finora
- Sexual Health FinalDocumento38 pagineSexual Health FinalRisna Dewi YantiNessuna valutazione finora
- Situation Analysis of Adolescent Sexual and Reproductive Health in the CaribbeanDocumento19 pagineSituation Analysis of Adolescent Sexual and Reproductive Health in the CaribbeanClaudia GonzalesNessuna valutazione finora
- Rates and barriers of HIV status disclosure among women in developing countriesDocumento9 pagineRates and barriers of HIV status disclosure among women in developing countriesTinkhaniMbichilaNessuna valutazione finora
- Adolescent and Youth Health ProgramDocumento11 pagineAdolescent and Youth Health ProgramVin Grace Tiqui - GuzmanNessuna valutazione finora
- Human Immunodeficiency Virus Care:: A Primary Care Provider's GuideDocumento18 pagineHuman Immunodeficiency Virus Care:: A Primary Care Provider's GuideMagaly AngelbaeNessuna valutazione finora
- Awareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolDocumento18 pagineAwareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolChristine Jean CeredonNessuna valutazione finora
- HIV/AIDS Awareness Evaluation in The Junior and Senior High School Students of University of The East Caloocan (UEC)Documento11 pagineHIV/AIDS Awareness Evaluation in The Junior and Senior High School Students of University of The East Caloocan (UEC)Sebastian Miguel CarlosNessuna valutazione finora
- Determinants of Youth Sexual Behaviour: Program Implications For IndiaDocumento9 pagineDeterminants of Youth Sexual Behaviour: Program Implications For IndiaUmanath R PoojaryNessuna valutazione finora
- Ias 16 4 18749Documento7 pagineIas 16 4 18749Amos AprekuNessuna valutazione finora
- Adherence To HIV Care and Associated Health Functioning Among Youth Living With HIV in Sub-Saharan AfricaDocumento15 pagineAdherence To HIV Care and Associated Health Functioning Among Youth Living With HIV in Sub-Saharan AfricaDouglas ChukwuNessuna valutazione finora
- Apc 2011 0025Documento10 pagineApc 2011 0025Stefania CristinaNessuna valutazione finora
- Department of Health - Adolescent and Youth Health Program (AYHP) - 2011-10-27Documento8 pagineDepartment of Health - Adolescent and Youth Health Program (AYHP) - 2011-10-27daryl ann dep-asNessuna valutazione finora
- Intimate Partner Violence Among Adolescents and Young Women - Prevalence and Associated Factors in Nine Countries - A Cross-Sectional Study PDFDocumento14 pagineIntimate Partner Violence Among Adolescents and Young Women - Prevalence and Associated Factors in Nine Countries - A Cross-Sectional Study PDFalkijohnNessuna valutazione finora
- MC For HIV Prevention Fact Sheet - 508Documento3 pagineMC For HIV Prevention Fact Sheet - 508Zunga MwaangaNessuna valutazione finora
- Hensel 2020Documento3 pagineHensel 2020AINANessuna valutazione finora
- USA HIV Statistics Among Youth 2012Documento4 pagineUSA HIV Statistics Among Youth 2012itzliehecatlNessuna valutazione finora
- Final Paper - HannahDocumento9 pagineFinal Paper - Hannahapi-457299309Nessuna valutazione finora
- Sexual Health MSMDocumento16 pagineSexual Health MSMShanti KarkiNessuna valutazione finora
- Childhood Sexual Abuse and Unsafe Sex Among Homosexual MenDocumento4 pagineChildhood Sexual Abuse and Unsafe Sex Among Homosexual MenSarwangNessuna valutazione finora
- HIV/AIDS Epidemiology in the 1980sDocumento2 pagineHIV/AIDS Epidemiology in the 1980selixNessuna valutazione finora
- Journal 2Documento8 pagineJournal 2Ryan Drake RomeroNessuna valutazione finora
- Christine Jean Ceridon-1 FINAL (Autosaved) - 1Documento40 pagineChristine Jean Ceridon-1 FINAL (Autosaved) - 1Christine Jean CeredonNessuna valutazione finora
- Gender Inequality in Hiv: Prevention Now, Programme Briefs, No. 4. 2002 UNFPADocumento5 pagineGender Inequality in Hiv: Prevention Now, Programme Briefs, No. 4. 2002 UNFPAPerkymeNessuna valutazione finora
- Within The Hidden Epidemic: Sexually Transmitted Diseases and HIV/AIDS Among American Indians and Alaska NativesDocumento11 pagineWithin The Hidden Epidemic: Sexually Transmitted Diseases and HIV/AIDS Among American Indians and Alaska NativesDarwinso AlvarezNessuna valutazione finora
- 11,12,13Documento14 pagine11,12,13Hedya Nadhrati SururaNessuna valutazione finora
- tmp65DD TMPDocumento9 paginetmp65DD TMPFrontiersNessuna valutazione finora
- tmp129F TMPDocumento9 paginetmp129F TMPFrontiersNessuna valutazione finora
- HIV and AIDS Risk Behaviors in Juvenile Detainees: Implications For Public Health PolicyDocumento7 pagineHIV and AIDS Risk Behaviors in Juvenile Detainees: Implications For Public Health PolicyGayatri Larasati0% (1)
- DohDocumento103 pagineDohRapSamputonNessuna valutazione finora
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsDa EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNessuna valutazione finora
- Heading Length Content: 2018 Policy Case Competition Presentation Guidelines 1. Executive SummaryDocumento2 pagineHeading Length Content: 2018 Policy Case Competition Presentation Guidelines 1. Executive SummaryJennNessuna valutazione finora
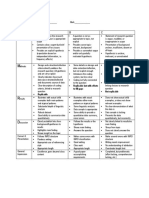
- Replicable But With Efforts To Fill Gaps Not ReplicableDocumento1 paginaReplicable But With Efforts To Fill Gaps Not ReplicableJennNessuna valutazione finora
- Co CurricularActivities TUEFA16Documento2 pagineCo CurricularActivities TUEFA16JennNessuna valutazione finora
- WCIG SupervisorForm Summer 2017Documento1 paginaWCIG SupervisorForm Summer 2017JennNessuna valutazione finora
- Apply for the Wasserman Center Internship Grant by February 23Documento3 pagineApply for the Wasserman Center Internship Grant by February 23JennNessuna valutazione finora
- Viewing GuideDocumento4 pagineViewing GuideJennNessuna valutazione finora
- WCIG SupervisorForm Summer 2017Documento1 paginaWCIG SupervisorForm Summer 2017JennNessuna valutazione finora
- Apply for the Wasserman Center Internship Grant by February 23Documento3 pagineApply for the Wasserman Center Internship Grant by February 23JennNessuna valutazione finora
- 2.6 Structure of DNA and RNADocumento11 pagine2.6 Structure of DNA and RNAJennNessuna valutazione finora
- Montgomery County Executive Hispanic Gala Educator of The Year Nomination FormDocumento1 paginaMontgomery County Executive Hispanic Gala Educator of The Year Nomination FormJennNessuna valutazione finora
- WCIG SupervisorForm Summer 2017Documento1 paginaWCIG SupervisorForm Summer 2017JennNessuna valutazione finora
- Estimating With Finite SumsDocumento18 pagineEstimating With Finite SumsJennNessuna valutazione finora
- 2.7 DNA Replication, Transcription, and TranslationDocumento25 pagine2.7 DNA Replication, Transcription, and TranslationJennNessuna valutazione finora
- School of Health and Allied Health Sciences Nursing DepartmentDocumento2 pagineSchool of Health and Allied Health Sciences Nursing DepartmentJuviely PremacioNessuna valutazione finora
- Implications of Early Pregnancy Obesity On Maternal, Fetal and Neonatal Health PDFDocumento7 pagineImplications of Early Pregnancy Obesity On Maternal, Fetal and Neonatal Health PDFAndhika Dimas ANessuna valutazione finora
- Call For Investigation Into Bill Gates 'Crimes Against Humanity' and 'Medical Malpractice' - Muslim MirrorDocumento2 pagineCall For Investigation Into Bill Gates 'Crimes Against Humanity' and 'Medical Malpractice' - Muslim Mirrorseanpa46473Nessuna valutazione finora
- Exposition EuthanasiaDocumento4 pagineExposition EuthanasiaHarman SainiNessuna valutazione finora
- Fiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1Documento133 pagineFiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1roddy narayanNessuna valutazione finora
- CA 2 - CHN Review 50 Items PretestDocumento10 pagineCA 2 - CHN Review 50 Items PretestAlibasher Macalnas100% (1)
- Schizophrenia: Table 1-DSM-IV-TR Diagnostic Criteria For SchizophreniaDocumento6 pagineSchizophrenia: Table 1-DSM-IV-TR Diagnostic Criteria For SchizophreniaNi Ti NNessuna valutazione finora
- SIR Epidemic Model Explained: Susceptible, Infected, Recovered PopulationsDocumento16 pagineSIR Epidemic Model Explained: Susceptible, Infected, Recovered Populationsmirast91Nessuna valutazione finora
- AssistDocumento90 pagineAssistMariam GugulashviliNessuna valutazione finora
- Hubungan Kondisi Lingkungan Fisik Rumah Dengan Kejadian Tuberkulosis Paru Di Jawa Barat (Analisis Data Riskesdas 2013)Documento6 pagineHubungan Kondisi Lingkungan Fisik Rumah Dengan Kejadian Tuberkulosis Paru Di Jawa Barat (Analisis Data Riskesdas 2013)Nova RizkenNessuna valutazione finora
- Pediatric History and Physical Exam TemplateDocumento4 paginePediatric History and Physical Exam TemplateJay Pee Tumaliuan Tumanguil0% (2)
- Essay EappDocumento1 paginaEssay EappAdrian BasasNessuna valutazione finora
- Mathematical Modelling of Infectious DiseasesDocumento11 pagineMathematical Modelling of Infectious DiseasesBOBBY212Nessuna valutazione finora
- National Immunization Program: Manual of Procedures Booklet 11Documento42 pagineNational Immunization Program: Manual of Procedures Booklet 11Blue PielagoNessuna valutazione finora
- Wins Accomplishment ReportDocumento4 pagineWins Accomplishment ReportSheila Marie Panulaya100% (5)
- COLD CHAIN & VaccinationDocumento40 pagineCOLD CHAIN & VaccinationHanif GandohNessuna valutazione finora
- Female Community Health Volunteer (FCHV) 3869130788167525523Documento38 pagineFemale Community Health Volunteer (FCHV) 3869130788167525523Xa UN MoychaNessuna valutazione finora
- Disease ProjectDocumento2 pagineDisease Projectsacann100% (1)
- Public Health Activities in Malaysia Throughout HistoryDocumento29 paginePublic Health Activities in Malaysia Throughout HistoryMohd Syis ZulkipliNessuna valutazione finora
- Emilio Aguinaldo College-Cavite: Communicable Diseases Among InfantsDocumento34 pagineEmilio Aguinaldo College-Cavite: Communicable Diseases Among Infantsarlian malihanNessuna valutazione finora
- NRHM MONTHLY PHC REPORTDocumento7 pagineNRHM MONTHLY PHC REPORTnaga vijayNessuna valutazione finora
- Infection and Bacterial InvasionDocumento40 pagineInfection and Bacterial InvasionTrisha BravoNessuna valutazione finora
- Bahasa Inggris: 250 Soal + PembahasanDocumento7 pagineBahasa Inggris: 250 Soal + Pembahasanfluos idNessuna valutazione finora
- Pandemic by Sonia ShahDocumento9 paginePandemic by Sonia ShahsimasNessuna valutazione finora
- Charter of DutiesDocumento3 pagineCharter of DutiesRezoan Ul IslamNessuna valutazione finora
- Lessons From The Miracle Doctors - Jon Barron - Ebook Medicine Health Cure Illness Healing Altern PDFDocumento176 pagineLessons From The Miracle Doctors - Jon Barron - Ebook Medicine Health Cure Illness Healing Altern PDFIrma Sari Muliadi100% (2)
- International Classification of Diseases (ICD 10)Documento5 pagineInternational Classification of Diseases (ICD 10)nk619466Nessuna valutazione finora
- Duties and Responsibilities of A Midwife in RhuDocumento6 pagineDuties and Responsibilities of A Midwife in RhuAlma PotenteNessuna valutazione finora
- REVIEW OF NATIONAL HEALTH MISSION & SDGSDocumento114 pagineREVIEW OF NATIONAL HEALTH MISSION & SDGSGargi pandeyNessuna valutazione finora
- Infection Control Practices in WorkplaceDocumento28 pagineInfection Control Practices in WorkplaceJames Patrick Dizon100% (1)