Potrebbero piacerti anche
- Neurodermatitis (Lichen Simplex Chronic) : ReferatDocumento12 pagineNeurodermatitis (Lichen Simplex Chronic) : ReferatJAQUELINENessuna valutazione finora
- Jurnal Anastesi 2Documento6 pagineJurnal Anastesi 2JAQUELINENessuna valutazione finora
- Morning Report: Abdominal TraumaDocumento10 pagineMorning Report: Abdominal TraumaJAQUELINENessuna valutazione finora
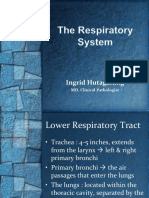
- Pengantar Sistem RespirasiDocumento23 paginePengantar Sistem RespirasiJAQUELINENessuna valutazione finora
- Praktikum Cardiovaskular DiseaseDocumento38 paginePraktikum Cardiovaskular DiseaseJAQUELINENessuna valutazione finora
- Viscosupplementation For Osteoarthritis of The KneeDocumento14 pagineViscosupplementation For Osteoarthritis of The KneeJAQUELINENessuna valutazione finora
- Jurnal 5Documento7 pagineJurnal 5JAQUELINENessuna valutazione finora
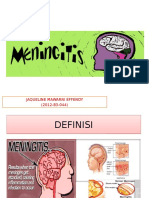
- Jaqueline Mawarni Effendy (2012-83-044)Documento15 pagineJaqueline Mawarni Effendy (2012-83-044)JAQUELINENessuna valutazione finora
- 2016 Article 1149Documento12 pagine2016 Article 1149JAQUELINENessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Wong YM 2018 Ryodoraku ShamDocumento3 pagineWong YM 2018 Ryodoraku Shamrswongym449100% (1)
- Adaptive Clinical Trials: September 27, 2006 Washington, D.C. FDA/Industry Statistics WorkshopDocumento169 pagineAdaptive Clinical Trials: September 27, 2006 Washington, D.C. FDA/Industry Statistics WorkshopRobMarvinNessuna valutazione finora
- Stem Cell ResearchDocumento3 pagineStem Cell Researchapi-236886045Nessuna valutazione finora
- ESA Medication-ErrorDocumento22 pagineESA Medication-ErrorMarius PapuricaNessuna valutazione finora
- Thesis Protocol FormatDocumento14 pagineThesis Protocol Formatsourabh jakharNessuna valutazione finora
- Studi Bioekivalensi Amoksisilin Generik Dan Dagang Menggunakan Matriks UrinDocumento7 pagineStudi Bioekivalensi Amoksisilin Generik Dan Dagang Menggunakan Matriks UrinEA12345aeNessuna valutazione finora
- Merckx 2017Documento17 pagineMerckx 2017Muhammad Imam NoorNessuna valutazione finora
- Med Safety WHO HIS SDS 2019.4 EngDocumento16 pagineMed Safety WHO HIS SDS 2019.4 Engdzipraz dziprazNessuna valutazione finora
- Tugas PharmaceuticalDocumento12 pagineTugas PharmaceuticalisnaeniNessuna valutazione finora
- Drug Registration and Essential DrugsDocumento42 pagineDrug Registration and Essential DrugsJeyanthakumar RasarathinamNessuna valutazione finora
- Jurnal FartokDocumento195 pagineJurnal FartokMustafa RahmatillahNessuna valutazione finora
- DOH HFSRB QOP 01 Form 2 3212019 postedDOHDocumento2 pagineDOH HFSRB QOP 01 Form 2 3212019 postedDOHMarcy100% (1)
- PHARMA 9 Trends and Issues in Nursing PharmacologyDocumento51 paginePHARMA 9 Trends and Issues in Nursing PharmacologyddsadNessuna valutazione finora
- QPS Pulmonary Respiratory SheetDocumento2 pagineQPS Pulmonary Respiratory SheetDenise van KampenNessuna valutazione finora
- SymHair Force 1631 QuickSheetDocumento4 pagineSymHair Force 1631 QuickSheetrafaeldelperu1982Nessuna valutazione finora
- Chapter 1: Structure and Composition: Independent Ethics CommitteeDocumento23 pagineChapter 1: Structure and Composition: Independent Ethics CommitteeBlissful DaysNessuna valutazione finora
- Wang2015 PDFDocumento11 pagineWang2015 PDFfriciliaNessuna valutazione finora
- PGDPHM Brochur 2019-20, Self SponsoredDocumento7 paginePGDPHM Brochur 2019-20, Self SponsoredsafetydmrcNessuna valutazione finora
- Clinical Oncology - Previous Examination Papers 2011Documento12 pagineClinical Oncology - Previous Examination Papers 2011wipi112Nessuna valutazione finora
- Ramani Mayappan Ramani@perlis - Uitm.edu - MyDocumento2 pagineRamani Mayappan Ramani@perlis - Uitm.edu - MyHasrolnizam HassanNessuna valutazione finora
- NCPDocumento3 pagineNCPmiguel_bernardo_5100% (1)
- Anterior Open Bite in The Mixed Dentition: European Journal of Paediatric Dentistry March 2019Documento4 pagineAnterior Open Bite in The Mixed Dentition: European Journal of Paediatric Dentistry March 2019TIFFANINessuna valutazione finora
- Instructions For Authors: Home Current Issue All Issues Browse By: CME Image Quizzes My JbjsDocumento5 pagineInstructions For Authors: Home Current Issue All Issues Browse By: CME Image Quizzes My JbjsdrorthokingNessuna valutazione finora
- Role of Biomedical EngineersDocumento240 pagineRole of Biomedical EngineersshodhgangaNessuna valutazione finora
- Abstract - Docx ALLDocumento138 pagineAbstract - Docx ALLvivekNessuna valutazione finora
- Effect of Intrathecal Hal.23Documento72 pagineEffect of Intrathecal Hal.23YayaNessuna valutazione finora
- Role of Chlorhexidine in Caries PreventionDocumento7 pagineRole of Chlorhexidine in Caries PreventionHarry ArdiyantoNessuna valutazione finora
- Ethics in Anaesthesia (June 2004) Write Briefly On Research Ethics (Dec 2008)Documento6 pagineEthics in Anaesthesia (June 2004) Write Briefly On Research Ethics (Dec 2008)Sirisha Ckv100% (1)
- Directory of Acredited Medical Testing LaboratoriesDocumento93 pagineDirectory of Acredited Medical Testing LaboratoriesCALIDAD METROMEDICA E.UNessuna valutazione finora
- The Accordion Pill: Presentation by Amirabbas SaffariDocumento11 pagineThe Accordion Pill: Presentation by Amirabbas SaffariAmirabbas SaffariNessuna valutazione finora