Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Juliana Tambellini: University of PittsburghDocumento19 pagineJuliana Tambellini: University of PittsburghtomeyttoNessuna valutazione finora
- Aplastik Anemia: Aplasia of Bone MarrowDocumento12 pagineAplastik Anemia: Aplasia of Bone MarrowtomeyttoNessuna valutazione finora
- 25A RA Changing Anaesthesia TrendsDocumento4 pagine25A RA Changing Anaesthesia TrendstomeyttoNessuna valutazione finora
- STYE (Hordeolum) : Frequent Signs and SymptomsDocumento1 paginaSTYE (Hordeolum) : Frequent Signs and SymptomstomeyttoNessuna valutazione finora
- Advances in Chest Drain Management in Thoracic DiseaseDocumento10 pagineAdvances in Chest Drain Management in Thoracic DiseasetomeyttoNessuna valutazione finora
- Reading of PartographDocumento33 pagineReading of PartographtomeyttoNessuna valutazione finora
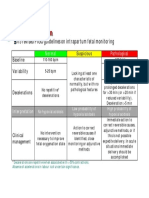
- CTG ClassificationDocumento1 paginaCTG ClassificationtomeyttoNessuna valutazione finora
- Fetal Death CH 13: 2009-2010 Academic Year MSIII Ob/Gyn Clerkship Self-Directed StudyDocumento12 pagineFetal Death CH 13: 2009-2010 Academic Year MSIII Ob/Gyn Clerkship Self-Directed StudytomeyttoNessuna valutazione finora
- Restaurant Safety EnglishDocumento25 pagineRestaurant Safety EnglishtomeyttoNessuna valutazione finora
- UveitisDocumento45 pagineUveitistomeytto100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Final DocumentDocumento49 pagineFinal Documentbernadette domoloanNessuna valutazione finora
- 100 Diseases Treated by Single Point of AcupunctureDocumento209 pagine100 Diseases Treated by Single Point of AcupunctureAgeng Rikhmawan100% (31)
- Prolapso de Cordón 1Documento10 pagineProlapso de Cordón 1Jhonatan MendozaNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaYuli ErmaNessuna valutazione finora
- Design 5 Hospital National Building CodeDocumento150 pagineDesign 5 Hospital National Building CodeRuzelAmpo-anNessuna valutazione finora
- Pressure Ulcer Prevention and Managment PolicyDocumento32 paginePressure Ulcer Prevention and Managment PolicybudimanNessuna valutazione finora
- CV FinalDocumento3 pagineCV FinalUrsi Adam Bacolod BahalaNessuna valutazione finora
- Carbetocin Versus Oxytocin For The Prevention of Postpartum Hemorrhage Following Elective Cesarean Section: Rizal Medical Center ExperienceDocumento46 pagineCarbetocin Versus Oxytocin For The Prevention of Postpartum Hemorrhage Following Elective Cesarean Section: Rizal Medical Center ExperienceShinta SariNessuna valutazione finora
- Personal Philosophy of NursingDocumento5 paginePersonal Philosophy of NursingsarahreyNessuna valutazione finora
- PreTest Obstetrics & Gynecology, Fifteenth EditionDocumento255 paginePreTest Obstetrics & Gynecology, Fifteenth EditionDr. Faeba JosephNessuna valutazione finora
- AbbreviationsDocumento3 pagineAbbreviationsJade Hemmings100% (1)
- Pre Auricular Sinus ReviewDocumento6 paginePre Auricular Sinus ReviewEthan LiaoNessuna valutazione finora
- EPDSScoringGuide March2015 PDFDocumento1 paginaEPDSScoringGuide March2015 PDFantivenomNessuna valutazione finora
- Neonatal Abstinence Syndrome Advances in Diagnosis and TreatmentDocumento14 pagineNeonatal Abstinence Syndrome Advances in Diagnosis and TreatmentdzratsoNessuna valutazione finora
- Dr. Victoria L. Batiquin and Allan Batiquin vs. Court of AppealsDocumento5 pagineDr. Victoria L. Batiquin and Allan Batiquin vs. Court of AppealsMykaNessuna valutazione finora
- Carboprost Drug StudyDocumento3 pagineCarboprost Drug StudyAjay SupanNessuna valutazione finora
- Ehs Hospital List For Both TG & ApDocumento43 pagineEhs Hospital List For Both TG & ApAvulaHarikrishnaYadavNessuna valutazione finora
- Matary Cases 2013Documento153 pagineMatary Cases 2013Raouf Ra'fat Soliman100% (10)
- Met Caz ClinicDocumento57 pagineMet Caz ClinicIndrecan AndreiNessuna valutazione finora
- Jurnal Bedah 11Documento20 pagineJurnal Bedah 11Andhyka Brillian KharismaNessuna valutazione finora
- Clincial Hours From TyphonDocumento6 pagineClincial Hours From Typhonapi-483862454Nessuna valutazione finora
- High School Argumentative Essay TopicsDocumento5 pagineHigh School Argumentative Essay Topicslpuaduwhd100% (2)
- Inguinal Hernias: Trix M. Asuncion M.D. General SurgeryDocumento55 pagineInguinal Hernias: Trix M. Asuncion M.D. General Surgeryjitendra magarNessuna valutazione finora
- Alraqi Medical Supply Company ProfileDocumento4 pagineAlraqi Medical Supply Company ProfileKaitlyn LewisNessuna valutazione finora
- MBFHI Self AppraisalDocumento26 pagineMBFHI Self AppraisalKarz KaraoNessuna valutazione finora
- Mechanism of Labour (Normal and Abnormal)Documento27 pagineMechanism of Labour (Normal and Abnormal)Rani100% (1)
- CME Miscarriages Combined 1Documento76 pagineCME Miscarriages Combined 1syawal zulfitriNessuna valutazione finora
- Yoga and Pranayama During High-Risk PregnancyDocumento7 pagineYoga and Pranayama During High-Risk PregnancyAdvanced Research PublicationsNessuna valutazione finora
- Principles of Casting and SplintingDocumento8 paginePrinciples of Casting and Splintingbobtaguba100% (1)
- Women'S Health and PoliciesDocumento10 pagineWomen'S Health and PoliciessamiaNessuna valutazione finora