Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Scientific Writing Made Easy: A Step-By - Step Guide To Undergraduate Writing in The Biological SciencesDocumento10 pagineScientific Writing Made Easy: A Step-By - Step Guide To Undergraduate Writing in The Biological SciencesArnab GhoshNessuna valutazione finora
- Scientific Writing Made Easy: A Step-By - Step Guide To Undergraduate Writing in The Biological SciencesDocumento10 pagineScientific Writing Made Easy: A Step-By - Step Guide To Undergraduate Writing in The Biological SciencesArnab GhoshNessuna valutazione finora
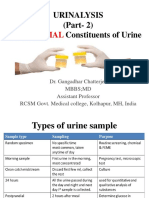
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocumento49 pagineUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNessuna valutazione finora
- Tribhuvan UniversityDocumento1 paginaTribhuvan UniversityArnab GhoshNessuna valutazione finora
- Digiscan - ListDocumento2 pagineDigiscan - ListArnab GhoshNessuna valutazione finora
- ModuleDocumento1 paginaModuleArnab GhoshNessuna valutazione finora
- Leukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Documento16 pagineLeukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Arnab Ghosh100% (1)
- General Approach in Investigation of Haemostasis: Coagulation InstrumentsDocumento24 pagineGeneral Approach in Investigation of Haemostasis: Coagulation InstrumentsArnab GhoshNessuna valutazione finora
- Adan-Flow Cytometry-Basic Principles and ApplicationsDocumento15 pagineAdan-Flow Cytometry-Basic Principles and ApplicationsArnab Ghosh100% (1)
- General Approach in Investigation of Haemostasis: Coagulation InstrumentsDocumento24 pagineGeneral Approach in Investigation of Haemostasis: Coagulation InstrumentsArnab GhoshNessuna valutazione finora
- Gurung Lho (Barga) PatroDocumento1 paginaGurung Lho (Barga) PatroArnab GhoshNessuna valutazione finora
- Final ICP AIPNA Int CME PathologyDocumento3 pagineFinal ICP AIPNA Int CME PathologyArnab GhoshNessuna valutazione finora
- 5 April 2016 - From Pramod To Write Dha Dont Write Haad 4 Examiners - Clin Path, Micro, Blood TransfusionDocumento1 pagina5 April 2016 - From Pramod To Write Dha Dont Write Haad 4 Examiners - Clin Path, Micro, Blood TransfusionArnab GhoshNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- He 3 Basic Types of Descriptive Research MethodsDocumento2 pagineHe 3 Basic Types of Descriptive Research MethodsRahul SarinNessuna valutazione finora
- Waste Heat Recovery UnitDocumento15 pagineWaste Heat Recovery UnitEDUARDONessuna valutazione finora
- (Cô Vũ Mai Phương) Tài liệu LIVESTREAM - Chuyên đề thi THPT - Câu hỏi giao tiếp xã hội (Buổi 1)Documento4 pagine(Cô Vũ Mai Phương) Tài liệu LIVESTREAM - Chuyên đề thi THPT - Câu hỏi giao tiếp xã hội (Buổi 1)nguyen duong trungNessuna valutazione finora
- Aakanksha ProjectDocumento32 pagineAakanksha ProjectAakash murarkaNessuna valutazione finora
- Constantino V MendezDocumento3 pagineConstantino V MendezNīc CādīgālNessuna valutazione finora
- Chapter 03Documento35 pagineChapter 03david jenil nabuaNessuna valutazione finora
- Handout Module6Documento69 pagineHandout Module6Oana MirceaNessuna valutazione finora
- E-Kabin - O Series - Monoblock Enclosure - ENGDocumento12 pagineE-Kabin - O Series - Monoblock Enclosure - ENGCatalina CocoşNessuna valutazione finora
- RMP ContractDocumento181 pagineRMP ContractHillary AmistosoNessuna valutazione finora
- Industries Visited in Pune & LonavalaDocumento13 pagineIndustries Visited in Pune & LonavalaRohan R Tamhane100% (1)
- Mdp36 The EndDocumento42 pagineMdp36 The Endnanog36Nessuna valutazione finora
- Maya Mendez ResumeDocumento2 pagineMaya Mendez Resumeapi-520985654Nessuna valutazione finora
- 10 Chapter 3 Occupancy Classification AnDocumento10 pagine10 Chapter 3 Occupancy Classification AnMatt BaronNessuna valutazione finora
- Tractor Price and Speci Cations: Tractors in IndiaDocumento4 pagineTractor Price and Speci Cations: Tractors in Indiatrupti kadamNessuna valutazione finora
- Form 28 Attendence RegisterDocumento1 paginaForm 28 Attendence RegisterSanjeet SinghNessuna valutazione finora
- E10b MERCHANT NAVY CODE OF CONDUCTDocumento1 paginaE10b MERCHANT NAVY CODE OF CONDUCTssabih75Nessuna valutazione finora
- Cis MSCMDocumento15 pagineCis MSCMOliver DimailigNessuna valutazione finora
- Gay Costa Del Sol - 2010Documento2 pagineGay Costa Del Sol - 2010gayinfospainNessuna valutazione finora
- Boeco BM-800 - User ManualDocumento21 pagineBoeco BM-800 - User ManualJuan Carlos CrespoNessuna valutazione finora
- Free Higher Education Application Form 1st Semester, SY 2021-2022Documento1 paginaFree Higher Education Application Form 1st Semester, SY 2021-2022Wheng NaragNessuna valutazione finora
- Cyber Safety PP Presentation For Class 11Documento16 pagineCyber Safety PP Presentation For Class 11WAZ CHANNEL100% (1)
- Legg Calve Perthes Disease: SynonymsDocumento35 pagineLegg Calve Perthes Disease: SynonymsAsad ChaudharyNessuna valutazione finora
- Plumbing Breakup M 01Documento29 paginePlumbing Breakup M 01Nicholas SmithNessuna valutazione finora
- Index Medicus PDFDocumento284 pagineIndex Medicus PDFVania Sitorus100% (1)
- Me N Mine Science X Ist TermDocumento101 pagineMe N Mine Science X Ist Termneelanshujain68% (19)
- BKM 10e Ch07 Two Security ModelDocumento2 pagineBKM 10e Ch07 Two Security ModelJoe IammarinoNessuna valutazione finora
- Argumentative Essay Research PaperDocumento5 pagineArgumentative Essay Research PaperJadNessuna valutazione finora
- 4 StartUp GuideDocumento2 pagine4 StartUp GuideSamuel RomeroNessuna valutazione finora
- Unit Weight of Soil in Quezon CityDocumento2 pagineUnit Weight of Soil in Quezon CityClarence Noel CorpuzNessuna valutazione finora
- Complaint: Employment Sexual Harassment Discrimination Against Omnicom & DDB NYDocumento38 pagineComplaint: Employment Sexual Harassment Discrimination Against Omnicom & DDB NYscl1116953Nessuna valutazione finora