Potrebbero piacerti anche
- Nac 2017Documento18 pagineNac 2017Nataly CortesNessuna valutazione finora
- Sepsis and Septic ShockDocumento4 pagineSepsis and Septic ShockFebyan AbotNessuna valutazione finora
- Communicablediseases 110227001506 Phpapp02 PDFDocumento30 pagineCommunicablediseases 110227001506 Phpapp02 PDFCrystal Ann Monsale TadiamonNessuna valutazione finora
- Abdominal Incisions and Sutures in Obstetrics and GynaecologyDocumento6 pagineAbdominal Incisions and Sutures in Obstetrics and GynaecologyFebyan AbotNessuna valutazione finora
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareDa EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNessuna valutazione finora
- 0221 Community-Acquired-PneumoniaDocumento29 pagine0221 Community-Acquired-PneumoniaDiego YanezNessuna valutazione finora
- Episiotomy ACOG PDFDocumento29 pagineEpisiotomy ACOG PDFFebyan AbotNessuna valutazione finora
- Neumonia Asociado A Servicios de La SaludDocumento7 pagineNeumonia Asociado A Servicios de La SaludOscarNessuna valutazione finora
- Ciz 1049Documento9 pagineCiz 1049Justin WilliemNessuna valutazione finora
- Comparison of Viral Infection in Healthcare-Associated Pneumonia (HCAP) and Community-Acquired Pneumonia (CAP)Documento16 pagineComparison of Viral Infection in Healthcare-Associated Pneumonia (HCAP) and Community-Acquired Pneumonia (CAP)MutianbllNessuna valutazione finora
- Community-Acquired Pneumonia - Strategies For Triage and Treatment. Cleveland Clinic 2020Documento7 pagineCommunity-Acquired Pneumonia - Strategies For Triage and Treatment. Cleveland Clinic 2020Gilberto GuzmanNessuna valutazione finora
- Comparison of Methicillin-Resistant Community-Acquired and Healthcare-Associated PneumoniaDocumento8 pagineComparison of Methicillin-Resistant Community-Acquired and Healthcare-Associated PneumoniaSuarniNessuna valutazione finora
- Chest: Health-Care-Associated Pneumonia Among Hospitalized Patients in A Japanese Community HospitalDocumento8 pagineChest: Health-Care-Associated Pneumonia Among Hospitalized Patients in A Japanese Community HospitalAndi BintangNessuna valutazione finora
- Community-Acquired Pneumonia: Strategies For Triage and TreatmentDocumento7 pagineCommunity-Acquired Pneumonia: Strategies For Triage and TreatmentAnita HeCasNessuna valutazione finora
- Choosing Antibiotic Therapy For Severe Community-Acquired PneumoniaDocumento7 pagineChoosing Antibiotic Therapy For Severe Community-Acquired PneumoniaJuan Sebastian SuarezNessuna valutazione finora
- Neumonia 2022Documento18 pagineNeumonia 2022Lele0407Nessuna valutazione finora
- New Guidelines For NeumoniaDocumento7 pagineNew Guidelines For NeumoniacarlosNessuna valutazione finora
- Nac Etiologia Implicacion para La Seleccion de La Poblacion Diseño de Estudios Cid 2008Documento4 pagineNac Etiologia Implicacion para La Seleccion de La Poblacion Diseño de Estudios Cid 2008Gustavo GomezNessuna valutazione finora
- Hospital-Acquired and Ventilator Associated Pneumonia Diagnosis, Management, and PreventionDocumento7 pagineHospital-Acquired and Ventilator Associated Pneumonia Diagnosis, Management, and PreventiontinatobingNessuna valutazione finora
- Hospital-Acquired andDocumento7 pagineHospital-Acquired andadhitiaNessuna valutazione finora
- BMJ 2021 065871.fullDocumento24 pagineBMJ 2021 065871.fullEfen YtNessuna valutazione finora
- Procalcitonin and AB DecisionsDocumento10 pagineProcalcitonin and AB DecisionsDennysson CorreiaNessuna valutazione finora
- Pneumonia: Etiology of Community-Acquired Pneumonia in Adults: A Systematic ReviewDocumento10 paginePneumonia: Etiology of Community-Acquired Pneumonia in Adults: A Systematic ReviewRizki Handayani SiregarNessuna valutazione finora
- Manejo de Neumonia en Pacientes CriticosDocumento24 pagineManejo de Neumonia en Pacientes CriticosMauricio Martinez HernandezNessuna valutazione finora
- Clinical Profile and Microbiological Aetiology Diagnosis in Adult Patients Hospitalized With Community-Acquired PneumoniaDocumento10 pagineClinical Profile and Microbiological Aetiology Diagnosis in Adult Patients Hospitalized With Community-Acquired PneumoniahajajNessuna valutazione finora
- 394 Full PDFDocumento20 pagine394 Full PDFHaltiNessuna valutazione finora
- Nac 10Documento12 pagineNac 10Emelyn FigueroaNessuna valutazione finora
- Ats-Idsa 2016 Hap VapDocumento51 pagineAts-Idsa 2016 Hap VapAlhafiz KarimNessuna valutazione finora
- Hap Vap Guidelines 2016 PDFDocumento51 pagineHap Vap Guidelines 2016 PDFJerryEddyaPutraBoerNessuna valutazione finora
- 2014 1 Moesm1 EsmDocumento51 pagine2014 1 Moesm1 EsmJesus RmNessuna valutazione finora
- Culture Negative SepsisDocumento5 pagineCulture Negative SepsismalvindersahiNessuna valutazione finora
- Personal View: Victor L YuDocumento5 paginePersonal View: Victor L Yudantheman123Nessuna valutazione finora
- Management of Pneumonia in Critically Ill Patients: Catia Cillóniz, Antoni Torres, Michael S NiedermanDocumento24 pagineManagement of Pneumonia in Critically Ill Patients: Catia Cillóniz, Antoni Torres, Michael S NiedermanMarvin Josue Bustamante GutierrezNessuna valutazione finora
- Jurnal 1Documento3 pagineJurnal 1RyuuzoraNessuna valutazione finora
- Procalcitonin 2Documento6 pagineProcalcitonin 2zivl1984Nessuna valutazione finora
- Diagnosis and Management of Community-Acquired Pneumonia: Evidence-Based PracticeDocumento11 pagineDiagnosis and Management of Community-Acquired Pneumonia: Evidence-Based PracticeMega Julia ThioNessuna valutazione finora
- Multiplex PCR Severe PneumoniaDocumento13 pagineMultiplex PCR Severe PneumoniaSrinivas PingaliNessuna valutazione finora
- Diagnostic and Prognostic Biomarkers of Sepsis in Critical CareDocumento8 pagineDiagnostic and Prognostic Biomarkers of Sepsis in Critical Caremr_curiousityNessuna valutazione finora
- Golden Hour CCM Arthur Van Zanten IC1Documento3 pagineGolden Hour CCM Arthur Van Zanten IC1Sara NicholsNessuna valutazione finora
- Methods of Cough AsessmentDocumento9 pagineMethods of Cough AsessmentDiogo TecelãoNessuna valutazione finora
- J Mayocp 2013 07 004Documento6 pagineJ Mayocp 2013 07 004Teh NuraqilahNessuna valutazione finora
- 10 1378@chest 123 5 1615Documento10 pagine10 1378@chest 123 5 1615SAYBLUs FANSNessuna valutazione finora
- Avances en Sepsis Art Ing 2022Documento10 pagineAvances en Sepsis Art Ing 2022roman rodriguezNessuna valutazione finora
- American Thoracic Society DocumentsDocumento29 pagineAmerican Thoracic Society DocumentsRci Club BucurestiNessuna valutazione finora
- tmpA70B TMPDocumento3 paginetmpA70B TMPFrontiersNessuna valutazione finora
- 2021 Article 6994Documento13 pagine2021 Article 6994Syrine BoughzalaNessuna valutazione finora
- Neumonia Asosiada A VentiladorDocumento11 pagineNeumonia Asosiada A VentiladorYnomata RusamellNessuna valutazione finora
- HCQ Study JamaDocumento7 pagineHCQ Study Jamathe kingfishNessuna valutazione finora
- Pittsburgh Lung Conference: PneumoniaDocumento4 paginePittsburgh Lung Conference: PneumoniaYudha Rental'sNessuna valutazione finora
- Association Between Immune-Related Adverse Event TDocumento8 pagineAssociation Between Immune-Related Adverse Event TAndrew FincoNessuna valutazione finora
- Antibiotico YPronosticoDocumento6 pagineAntibiotico YPronosticoagonzale52Nessuna valutazione finora
- Bacterial Meningitis Guidelines IDSADocumento18 pagineBacterial Meningitis Guidelines IDSAAldito GlasgowNessuna valutazione finora
- Ultra-Short Course Antibiotics For Pneumonia With Preserved OxygenationDocumento2 pagineUltra-Short Course Antibiotics For Pneumonia With Preserved Oxygenationapi-648891519Nessuna valutazione finora
- Improved Survival Among Icu-Hospitalized Patients With Community-Acquired Pneumonia by Unidentified Organisms: A Multicenter Case-Control StudyDocumento12 pagineImproved Survival Among Icu-Hospitalized Patients With Community-Acquired Pneumonia by Unidentified Organisms: A Multicenter Case-Control Studysigit_ananda07Nessuna valutazione finora
- Procalcitoninandcap PDFDocumento10 pagineProcalcitoninandcap PDFmohd zonNessuna valutazione finora
- Clinical Practice Guideline For The Use of Antimicrobial Agents in Neutropenic Patients With CancerDocumento38 pagineClinical Practice Guideline For The Use of Antimicrobial Agents in Neutropenic Patients With CancerAini Sofa HaniahNessuna valutazione finora
- Ventilator AssociatedDocumento10 pagineVentilator Associatedtoothfairy2780Nessuna valutazione finora
- Use of Flexible Bronchoscopy in The Diagnosis of Infectious Etiologies - A Literature ReviewDocumento4 pagineUse of Flexible Bronchoscopy in The Diagnosis of Infectious Etiologies - A Literature ReviewAna MercadoNessuna valutazione finora
- The Evidence Supporting The Revised EORTC-MSGERC Definitions For Invasive Fungal InfectionsDocumento2 pagineThe Evidence Supporting The Revised EORTC-MSGERC Definitions For Invasive Fungal Infectionsgwyneth.green.512Nessuna valutazione finora
- Hap+vap Ats - Idsa 2016 (01-20)Documento20 pagineHap+vap Ats - Idsa 2016 (01-20)rahayuNessuna valutazione finora
- 10 1056@NEJMoa1812379Documento12 pagine10 1056@NEJMoa1812379alvaroNessuna valutazione finora
- Validacion CPISDocumento5 pagineValidacion CPISXavier AbrilNessuna valutazione finora
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumDa EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNessuna valutazione finora
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19Da EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19Nessuna valutazione finora
- Inflammation: The Common Pathway of Stress-Related Diseases: Yun-Zi Liu Yun-Xia Wang Chun-Lei JiangDocumento11 pagineInflammation: The Common Pathway of Stress-Related Diseases: Yun-Zi Liu Yun-Xia Wang Chun-Lei JiangFebyan AbotNessuna valutazione finora
- Controlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksDocumento27 pagineControlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksFebyan AbotNessuna valutazione finora
- NPP 2013297 ADocumento8 pagineNPP 2013297 AFebyan AbotNessuna valutazione finora
- Combination of PPI With A Prokinetic Drug in Gastroesophageal Reflux DiseaseDocumento19 pagineCombination of PPI With A Prokinetic Drug in Gastroesophageal Reflux DiseaseFebyan AbotNessuna valutazione finora
- Controlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksDocumento27 pagineControlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksFebyan AbotNessuna valutazione finora
- Editorial: Stress Induced Neuroplasticity and Mental DisordersDocumento4 pagineEditorial: Stress Induced Neuroplasticity and Mental DisordersFebyan AbotNessuna valutazione finora
- 10 1016@j Psyneuen 2017 09 007Documento43 pagine10 1016@j Psyneuen 2017 09 007Febyan AbotNessuna valutazione finora
- Mud I Gonda 2013Documento3 pagineMud I Gonda 2013Febyan AbotNessuna valutazione finora
- Salicil Acid DermaDocumento9 pagineSalicil Acid DermaFebyan AbotNessuna valutazione finora
- VitiligoDocumento13 pagineVitiligoFebyan AbotNessuna valutazione finora
- Endoscopy in The ElderlyDocumento7 pagineEndoscopy in The ElderlyFebyan AbotNessuna valutazione finora
- Tulisan Nyeri Saraf Adelyna MelialaDocumento5 pagineTulisan Nyeri Saraf Adelyna MelialaFebyan AbotNessuna valutazione finora
- Review Article: Signal Transductions and Nonalcoholic Fatty Liver: A Mini-ReviewDocumento8 pagineReview Article: Signal Transductions and Nonalcoholic Fatty Liver: A Mini-ReviewFebyan AbotNessuna valutazione finora
- Journal of Molecular SignalingDocumento11 pagineJournal of Molecular SignalingFebyan AbotNessuna valutazione finora
- 25122012012424Documento6 pagine25122012012424Febyan AbotNessuna valutazione finora
- JP 05008Documento6 pagineJP 05008Febyan AbotNessuna valutazione finora
- Green Tea Polyphenol Epigallocatechin-3-Gallate Ameliorates Insulin Resistance in Non-Alcoholic Fatty Liver Disease MiceDocumento9 pagineGreen Tea Polyphenol Epigallocatechin-3-Gallate Ameliorates Insulin Resistance in Non-Alcoholic Fatty Liver Disease MiceFebyan AbotNessuna valutazione finora
- Reasons For Routine Episiotomy A Mixed Methods Study in A Large Maternity Hospital in Phnom Penh CambodiaDocumento11 pagineReasons For Routine Episiotomy A Mixed Methods Study in A Large Maternity Hospital in Phnom Penh CambodiaFebyan AbotNessuna valutazione finora
- Seijmonsbergenschermers 2013Documento9 pagineSeijmonsbergenschermers 2013Febyan AbotNessuna valutazione finora
- 1 PB PDFDocumento8 pagine1 PB PDFFebyan AbotNessuna valutazione finora
- Material Safety Data Sheet: 1. Identification of The Substance/Preparation and The Company/UndertakingDocumento9 pagineMaterial Safety Data Sheet: 1. Identification of The Substance/Preparation and The Company/UndertakingFebyan AbotNessuna valutazione finora
- Zika Virus: Emerging Arboviral Threat To BangladeshDocumento17 pagineZika Virus: Emerging Arboviral Threat To BangladeshlkokodkodNessuna valutazione finora
- Jurnal BaliDocumento25 pagineJurnal BaliIndah ParwatiNessuna valutazione finora
- The Most Dangerous in HistoryDocumento10 pagineThe Most Dangerous in HistorymausanpraNessuna valutazione finora
- The Impact of Covid-19 On RestaurantsDocumento4 pagineThe Impact of Covid-19 On RestaurantsIJRASETPublicationsNessuna valutazione finora
- HIV/AIDS Cases in Region III (Central Luzon) : Epidemiology BureauDocumento8 pagineHIV/AIDS Cases in Region III (Central Luzon) : Epidemiology BureauMHO Ng DRT BulacanNessuna valutazione finora
- Mastermind: WorksheetDocumento23 pagineMastermind: WorksheetMilka RahmanNessuna valutazione finora
- Coronavirus Disease 2020 (COVID-19) : China National Pharmaceutical Group Co - LTD (SINOPHARM)Documento20 pagineCoronavirus Disease 2020 (COVID-19) : China National Pharmaceutical Group Co - LTD (SINOPHARM)Anusheh Asad100% (1)
- MicrobiologyDocumento17 pagineMicrobiologykimacol659Nessuna valutazione finora
- Dengue-WPS OfficeDocumento20 pagineDengue-WPS OfficeAnnamalai MNessuna valutazione finora
- Tricho MoniasisDocumento38 pagineTricho MoniasisAkhmad Ikhwan BaidlowiNessuna valutazione finora
- List of Viruses Covered Under NCS-TCPDocumento5 pagineList of Viruses Covered Under NCS-TCPmanojbanNessuna valutazione finora
- NSTP 2 Unit 4 and 5 ReviewerDocumento11 pagineNSTP 2 Unit 4 and 5 ReviewerSophie DatuNessuna valutazione finora
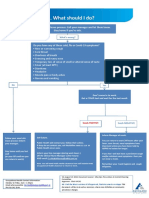
- What To Do If Youre Sick FlowchartDocumento1 paginaWhat To Do If Youre Sick FlowchartfuckyouNessuna valutazione finora
- SSI: Abx Treatment & ManagementDocumento26 pagineSSI: Abx Treatment & ManagementSalsabila Al-BasheerNessuna valutazione finora
- Aids 2Documento2 pagineAids 2Ausberto IbañezNessuna valutazione finora
- Etextbook 978 0134019192 Microbiology With Diseases by TaxonomyDocumento62 pagineEtextbook 978 0134019192 Microbiology With Diseases by Taxonomylashawn.fain938100% (48)
- Eritrasma 2012Documento17 pagineEritrasma 2012Ammar HasyimNessuna valutazione finora
- 0000 0000:Dr Manlapig MergedDocumento51 pagine0000 0000:Dr Manlapig MergedAj Christian Lacuesta IsipNessuna valutazione finora
- Health Declaration Form A1 Whole PageDocumento1 paginaHealth Declaration Form A1 Whole PageMiamor NatividadNessuna valutazione finora
- Ch. 23 Infectious DiseasesDocumento40 pagineCh. 23 Infectious Diseases吴昊Nessuna valutazione finora
- Blood and Tissue ParasitesDocumento62 pagineBlood and Tissue Parasitesapi-3856362Nessuna valutazione finora
- URI Case (2 Lab Lecture) Patient Presentation: Chief ComplaintDocumento2 pagineURI Case (2 Lab Lecture) Patient Presentation: Chief ComplaintMOHANNADNessuna valutazione finora
- Return Permit For Resident Outside UAEDocumento3 pagineReturn Permit For Resident Outside UAEᘉᓋᘻᗗᘙ ᘉᓋᙏᓲ ᖽᐸᗁᕠᘘNessuna valutazione finora
- Assess and Classify The Sick Child Age 2 Months Up To 5 YearsDocumento76 pagineAssess and Classify The Sick Child Age 2 Months Up To 5 YearsTaniaNessuna valutazione finora
- Antibiotic Prophylaxis OrthoDocumento4 pagineAntibiotic Prophylaxis OrthoDonNessuna valutazione finora
- A Mathematical ModelDocumento4 pagineA Mathematical ModelInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Microbial Disease of Respiratory SystemDocumento2 pagineMicrobial Disease of Respiratory SystemJanah AbucayNessuna valutazione finora
- Sangguniang Panlungsod: Republic of The PhilippinesDocumento2 pagineSangguniang Panlungsod: Republic of The PhilippinesClarisse Marion DenilaNessuna valutazione finora
- Muffakham Jah: College of Engineering and TechnologyDocumento2 pagineMuffakham Jah: College of Engineering and Technologymrcopy xeroxNessuna valutazione finora