Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- INFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Documento21 pagineINFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Si PuputNessuna valutazione finora
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocumento14 pagineRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNessuna valutazione finora
- Eye Health in The Commonwealth - Progress Report 2018 To 2020Documento30 pagineEye Health in The Commonwealth - Progress Report 2018 To 2020Si PuputNessuna valutazione finora
- Current Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathyDocumento11 pagineCurrent Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathySi PuputNessuna valutazione finora
- Towards Universal Eye Health Western PacificDocumento28 pagineTowards Universal Eye Health Western PacificSi PuputNessuna valutazione finora
- Normal Postnatal Ocular DevelopmentDocumento23 pagineNormal Postnatal Ocular DevelopmentSi PuputNessuna valutazione finora
- Duty Report 18 Januari 2020Documento13 pagineDuty Report 18 Januari 2020Si PuputNessuna valutazione finora
- Rapid Sequence InductionDocumento2 pagineRapid Sequence InductionSi PuputNessuna valutazione finora
- New Doc 2018-05-04Documento2 pagineNew Doc 2018-05-04Si PuputNessuna valutazione finora
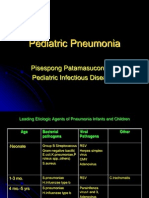
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDocumento39 paginePediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Shen-Hammer Pulse Diagnosis and Overgrowth of CandidaDocumento4 pagineShen-Hammer Pulse Diagnosis and Overgrowth of CandidaRocío JMNessuna valutazione finora
- 04IJPHY907Documento8 pagine04IJPHY907ize browniezNessuna valutazione finora
- LGBT Issues in TherapyDocumento2 pagineLGBT Issues in TherapyChelsea DeanNessuna valutazione finora
- Care and Maintenance To Reduce Vascular Access ComplicationsDocumento98 pagineCare and Maintenance To Reduce Vascular Access ComplicationsAgnes BastonNessuna valutazione finora
- Intravenous Fluid Guideline-1Documento4 pagineIntravenous Fluid Guideline-1Marco CalvaraNessuna valutazione finora
- Child Art Therapy (PDFDrive)Documento467 pagineChild Art Therapy (PDFDrive)Ilsu Pamuk100% (5)
- Oral & Craniofascial PainDocumento36 pagineOral & Craniofascial PainMaria Fudji hastutiNessuna valutazione finora
- Biology Investigatory Parkinson's PDFDocumento16 pagineBiology Investigatory Parkinson's PDFaneesh100% (2)
- Dr. Shoeb MujawarDocumento4 pagineDr. Shoeb Mujawarmeena syedNessuna valutazione finora
- Perioral DermatitisDocumento5 paginePerioral DermatitisAstriana IndrawatiNessuna valutazione finora
- Pain ManagementDocumento8 paginePain Managementmheng_a90Nessuna valutazione finora
- Non-Invasive Handheld Trans Cutaneous Bilirubinometer-FinalDocumento17 pagineNon-Invasive Handheld Trans Cutaneous Bilirubinometer-Finalarchana_jayarajNessuna valutazione finora
- Introduction Creation TherapyDocumento3 pagineIntroduction Creation TherapyRoger YoungNessuna valutazione finora
- A.S.P.E.N. Clinical Guidelines: Nutrition Support in Adult Acute and Chronic Renal FailureDocumento12 pagineA.S.P.E.N. Clinical Guidelines: Nutrition Support in Adult Acute and Chronic Renal FailureCarlos RaiolNessuna valutazione finora
- Exam in MS1 Cope 2nd ExamDocumento5 pagineExam in MS1 Cope 2nd ExamIbrahim RegachoNessuna valutazione finora
- Children and Trauma A YUENDocumento16 pagineChildren and Trauma A YUENMaría Soledad LatorreNessuna valutazione finora
- NCP For Chronic PainDocumento11 pagineNCP For Chronic PainRYAN SAPLADNessuna valutazione finora
- Soapp RDocumento7 pagineSoapp RAnaaaerobios100% (1)
- Malignant Soft Tissue TumorsDocumento21 pagineMalignant Soft Tissue TumorsEva GustianiNessuna valutazione finora
- Acute Spinal Cord InjuryDocumento3 pagineAcute Spinal Cord InjuryMarisol Dellera ValmoriaNessuna valutazione finora
- Fundamentals Exam ADocumento38 pagineFundamentals Exam APatrice Miller100% (3)
- Kim Ngoc Nguyen (21859825) - Reflective EssayDocumento1 paginaKim Ngoc Nguyen (21859825) - Reflective EssaynkngocNessuna valutazione finora
- What Is DementiaDocumento5 pagineWhat Is DementiaKaren Kenneth BonotanNessuna valutazione finora
- Medical Records in Family PracticeDocumento22 pagineMedical Records in Family PracticenurfadillahNessuna valutazione finora
- Asia Pacific Occupational Therapy Congress ProgrammeDocumento8 pagineAsia Pacific Occupational Therapy Congress ProgrammeRLedgerdNessuna valutazione finora
- ThalidomideDocumento5 pagineThalidomideVarun HVNessuna valutazione finora
- Neonatal RN Resume Level III Neonatal ICU Dallas TX OnlyDocumento3 pagineNeonatal RN Resume Level III Neonatal ICU Dallas TX OnlyRick Whitley100% (3)
- Fever PresentationDocumento15 pagineFever PresentationMaira InaamNessuna valutazione finora
- Medical Emergencies OMFSDocumento72 pagineMedical Emergencies OMFSkatnev100% (1)
- Acupuncture For Body 1 10Documento10 pagineAcupuncture For Body 1 10mamun310% (1)