Potrebbero piacerti anche
- Oman New Reimbursement Claim FormDocumento3 pagineOman New Reimbursement Claim Formtoalok4723Nessuna valutazione finora
- Mental Illness and HomelessnessDocumento2 pagineMental Illness and HomelessnessLauren FaustNessuna valutazione finora
- Cure For Schizophrenia A Journey Can Biological Control Systems Be The Answer To Chemical Regulation?Documento54 pagineCure For Schizophrenia A Journey Can Biological Control Systems Be The Answer To Chemical Regulation?Mushahid100% (1)
- Medical ImagingDocumento8 pagineMedical ImagingMansourNessuna valutazione finora
- Holistic VillageDocumento5 pagineHolistic VillagemeghadurganNessuna valutazione finora
- CPG Abnormal Labor and Delivery PDFDocumento29 pagineCPG Abnormal Labor and Delivery PDFKarl Jimenez Separa100% (2)
- LUTRONIC 2020 CataolgDocumento13 pagineLUTRONIC 2020 Cataolgkhairul ihsanNessuna valutazione finora
- Central Auditory PathwaysDocumento31 pagineCentral Auditory Pathwayslion2chNessuna valutazione finora
- Dementia Nursing Care PlanDocumento2 pagineDementia Nursing Care PlanCyrus De Asis95% (19)
- Management of Failed Block - Harsh.Documento48 pagineManagement of Failed Block - Harsh.Faeiz KhanNessuna valutazione finora
- Wastewater Treatment Advanced PDFDocumento368 pagineWastewater Treatment Advanced PDFradoineNessuna valutazione finora
- Dialysis Centre: Assignment - 3Documento12 pagineDialysis Centre: Assignment - 3grvoneandonlyNessuna valutazione finora
- Treatment-Resistant Obsessive-Compulsive Disorder (OCD) - Current UnderstandingDocumento21 pagineTreatment-Resistant Obsessive-Compulsive Disorder (OCD) - Current UnderstandingRapapportNessuna valutazione finora
- Thyroid Carcinoma Case PreDocumento22 pagineThyroid Carcinoma Case PreTabrrett Bethel100% (1)
- Parkinson's DiseaseDocumento17 pagineParkinson's DiseaseRafael Carrillo-BaylonNessuna valutazione finora
- Addison's DiseaseDocumento17 pagineAddison's DiseaseMah Jezthy100% (1)
- Novel Pharmacological Targets For The Treatment of Parkinson's DiseaseDocumento10 pagineNovel Pharmacological Targets For The Treatment of Parkinson's Disease2013_10_33_03_11_164Nessuna valutazione finora
- Herbal Treatment of Parkinsonism A ReviewDocumento7 pagineHerbal Treatment of Parkinsonism A ReviewKartika BorraNessuna valutazione finora
- Stem Cell-Based Therapies For Parkinson DiseaseDocumento17 pagineStem Cell-Based Therapies For Parkinson DiseaseYunita Christiani BiyangNessuna valutazione finora
- AANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseDocumento6 pagineAANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseMarianne GarciaNessuna valutazione finora
- 1423 0127 17 4Documento10 pagine1423 0127 17 4Miguel Angel Santillàn VàzquezNessuna valutazione finora
- Characterization of Cognitive Deficits in Rats Overexpressing Human Alpha-Synuclein in The Ventral Tegmental Area and Medial Septum Using Recombinant Adeno-Associated Viral Vectors (2013)Documento12 pagineCharacterization of Cognitive Deficits in Rats Overexpressing Human Alpha-Synuclein in The Ventral Tegmental Area and Medial Septum Using Recombinant Adeno-Associated Viral Vectors (2013)Rifqi Fathul ArroisiNessuna valutazione finora
- Transmitters and Disorders HandoutDocumento3 pagineTransmitters and Disorders HandoutfrazzycakebossNessuna valutazione finora
- Caffeine As A Pharmacological ToolDocumento5 pagineCaffeine As A Pharmacological ToolNala Dwi HartatiNessuna valutazione finora
- Learning Objectives For The Pharmacology of Parkinson Disease Drugs.Documento5 pagineLearning Objectives For The Pharmacology of Parkinson Disease Drugs.bl9nkverseNessuna valutazione finora
- Parkinson's Disease: Mechanisms, Translational Models and Management StrategiesDocumento14 pagineParkinson's Disease: Mechanisms, Translational Models and Management StrategiesGleyce CabralNessuna valutazione finora
- NDT 5190 Therapeutic Interventions and Adjustments in The Management 072910Documento8 pagineNDT 5190 Therapeutic Interventions and Adjustments in The Management 072910MatejNessuna valutazione finora
- Schapira - v7 - DY - FinalDocumento46 pagineSchapira - v7 - DY - FinalTamimjdNessuna valutazione finora
- Cognitive and Behavioral Disorders in Parkinson's Disease (2017)Documento9 pagineCognitive and Behavioral Disorders in Parkinson's Disease (2017)LaureanoNessuna valutazione finora
- TMP - 4306 300 596 1 SM (3) 1791561448Documento5 pagineTMP - 4306 300 596 1 SM (3) 1791561448Lulu LuwiiNessuna valutazione finora
- El Eje Intestinal-Cerebral en La Enfermedad de Parkinson - Posibilidades para Terapias Basadas en AlimentosDocumento10 pagineEl Eje Intestinal-Cerebral en La Enfermedad de Parkinson - Posibilidades para Terapias Basadas en Alimentosjaviera vergaraNessuna valutazione finora
- Jurding JiwaDocumento8 pagineJurding JiwaAliRifqiAlkaffNessuna valutazione finora
- Non-Motor Symptoms in Atypical Parkinsonian SyndromesDocumento21 pagineNon-Motor Symptoms in Atypical Parkinsonian Syndromesנועה פרץNessuna valutazione finora
- Aringhieri 2018Documento92 pagineAringhieri 2018Mariana PestanaNessuna valutazione finora
- 5422 FullDocumento10 pagine5422 FullEkeleme Nnamdi MartinsNessuna valutazione finora
- Toneuj 10 42 PDFDocumento17 pagineToneuj 10 42 PDFpratiwifatmasariNessuna valutazione finora
- 10 - PHAR0004 - 9 - 7 Adrenergics - 2 - RB - 2018 - NotesDocumento4 pagine10 - PHAR0004 - 9 - 7 Adrenergics - 2 - RB - 2018 - NotesArthi ArumukasamyNessuna valutazione finora
- Journal of Neurochemistry - 2011 - Jafari - Structural Contributions of Antipsychotic Drugs To Their Therapeutic ProfilesDocumento14 pagineJournal of Neurochemistry - 2011 - Jafari - Structural Contributions of Antipsychotic Drugs To Their Therapeutic Profilesjohnny chawNessuna valutazione finora
- Drug-Induced Parkinsonism: Hae-Won Shin, Sun Ju ChungDocumento7 pagineDrug-Induced Parkinsonism: Hae-Won Shin, Sun Ju ChungBaskarazrNessuna valutazione finora
- TMP FFC1Documento28 pagineTMP FFC1FrontiersNessuna valutazione finora
- Spektro Uv VisDocumento7 pagineSpektro Uv VisNadaNessuna valutazione finora
- Parkinson's Disease: Neurovascular DisordersDocumento24 pagineParkinson's Disease: Neurovascular DisordersNdoo NdooNessuna valutazione finora
- Animal Model of EADocumento13 pagineAnimal Model of EAzigurat00Nessuna valutazione finora
- Parkinson and Gambling ExampleDocumento4 pagineParkinson and Gambling ExampleAlexandra IonelaNessuna valutazione finora
- Neurophysiology of Depression and Bipolar Affective DisorderDocumento17 pagineNeurophysiology of Depression and Bipolar Affective DisorderShivan A.C.Nessuna valutazione finora
- Extrapyramidal Symptoms - StatPearls - NCBI BookshelfDocumento6 pagineExtrapyramidal Symptoms - StatPearls - NCBI BookshelfFitrah RahmadhaniNessuna valutazione finora
- Articles:: Q&A: Q&A: Dear SIRSDocumento5 pagineArticles:: Q&A: Q&A: Dear SIRSLucy WijayaNessuna valutazione finora
- Abstract - NaKATPase e ParkinsonDocumento1 paginaAbstract - NaKATPase e Parkinsongeorgia santosNessuna valutazione finora
- 2019 European Academy of Neurology Parkinson DiseaseDocumento16 pagine2019 European Academy of Neurology Parkinson DiseaseJuan Diego Gutierrez ZevallosNessuna valutazione finora
- s41380 021 01384 8Documento10 pagines41380 021 01384 8mariamojegNessuna valutazione finora
- 6 Vol. 10 Issue 11 Nov 2019 IJPSR RA 11687Documento7 pagine6 Vol. 10 Issue 11 Nov 2019 IJPSR RA 11687Charles OnunekwuNessuna valutazione finora
- Parkinson's: A Syndrome Rather Than A Disease?: BackgroundDocumento8 pagineParkinson's: A Syndrome Rather Than A Disease?: BackgroundEduardo Santana SuárezNessuna valutazione finora
- The Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiDocumento20 pagineThe Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiTherezia Sonia Gabriella TanggulunganNessuna valutazione finora
- Bangsal Ganglia A New Therapy ParkinsonDocumento4 pagineBangsal Ganglia A New Therapy ParkinsonekaamirudienNessuna valutazione finora
- Dr. Esmie T. Agpalo Alfie C. Ballesteros: NeurotransmittersDocumento4 pagineDr. Esmie T. Agpalo Alfie C. Ballesteros: NeurotransmittersAlfie Clores BallesterosNessuna valutazione finora
- Epigenetic Inactivation of The Autophagy - Lysosomal System in Appendix in Parkinson 'S DiseaseDocumento18 pagineEpigenetic Inactivation of The Autophagy - Lysosomal System in Appendix in Parkinson 'S DiseaseOliwia MalonNessuna valutazione finora
- Article Ejbps Volume 6 August Issue 8 1564793897Documento8 pagineArticle Ejbps Volume 6 August Issue 8 1564793897Rashid IqbalNessuna valutazione finora
- 3.current Pharmaceutical Treatments and Alternative Therapies ofDocumento17 pagine3.current Pharmaceutical Treatments and Alternative Therapies ofPaula Betancor MontesdeocaNessuna valutazione finora
- Background Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingDocumento27 pagineBackground Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingCharan Pal SinghNessuna valutazione finora
- The Metabotropic Purinergic P2Y Receptor Family As Novel Drug Target in EpilepsyDocumento12 pagineThe Metabotropic Purinergic P2Y Receptor Family As Novel Drug Target in EpilepsymhcolinaNessuna valutazione finora
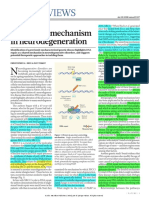
- News & Views: A Unifying Mechanism in NeurodegenerationDocumento2 pagineNews & Views: A Unifying Mechanism in Neurodegenerationrocambolescas perthNessuna valutazione finora
- Dopa RewardDocumento8 pagineDopa RewardDenia Méndez ÁlvarezNessuna valutazione finora
- Effect of Walking Along Circle On Foot Prints in Parkinson's On FreezingDocumento48 pagineEffect of Walking Along Circle On Foot Prints in Parkinson's On FreezingAnup ShankarwarNessuna valutazione finora
- Caripirazine Compared To Aripiprazole in PCP Induced Attention DeficitsDocumento12 pagineCaripirazine Compared To Aripiprazole in PCP Induced Attention DeficitsEsraa SaeedNessuna valutazione finora
- Weil - Cholinergic System Changes in Parkinson - PlainText - CleanDocumento25 pagineWeil - Cholinergic System Changes in Parkinson - PlainText - CleanLên DươngNessuna valutazione finora
- Ezqui y DopaDocumento7 pagineEzqui y DopaJuanAmayaNessuna valutazione finora
- Role of Neuro Imagine WindhorstDocumento69 pagineRole of Neuro Imagine Windhorstzendah123Nessuna valutazione finora
- AnandDocumento12 pagineAnandre septian IlhamsyahNessuna valutazione finora
- 2013 Adenosine Signaling in Striatal Circuits and AUDDocumento8 pagine2013 Adenosine Signaling in Striatal Circuits and AUDMuhammad Sona KhanNessuna valutazione finora
- Content ServerDocumento11 pagineContent ServerHendi Imam RamadhanNessuna valutazione finora
- Detection of K-Complexes and Sleep Spindles (DETOKS) Using Sparse OptimizationDocumento12 pagineDetection of K-Complexes and Sleep Spindles (DETOKS) Using Sparse OptimizationLulu Luwii0% (1)
- EEG 2010 Pitfalls in EEG Interpretation-Anannit HODocumento13 pagineEEG 2010 Pitfalls in EEG Interpretation-Anannit HOLulu LuwiiNessuna valutazione finora
- Transcranial Doppler Sonography Pulsatility Index (PI) Reflects Intracranial Pressure (ICP)Documento7 pagineTranscranial Doppler Sonography Pulsatility Index (PI) Reflects Intracranial Pressure (ICP)Lulu LuwiiNessuna valutazione finora
- Complex Gangliosides As Autoantibody Targets at The Neuromuscular Junction in Miller Fisher Syndrome: A Current PerspectiveDocumento13 pagineComplex Gangliosides As Autoantibody Targets at The Neuromuscular Junction in Miller Fisher Syndrome: A Current PerspectiveLulu LuwiiNessuna valutazione finora
- Korelasi Ekspresi VEGF Dan Densitas Mikrovesel Dengan Respons Radioterapi Adenokarsinoma ServiksDocumento11 pagineKorelasi Ekspresi VEGF Dan Densitas Mikrovesel Dengan Respons Radioterapi Adenokarsinoma ServiksLulu LuwiiNessuna valutazione finora
- Brainedema 160314142234Documento39 pagineBrainedema 160314142234Lulu LuwiiNessuna valutazione finora
- Spinal Cord and Reflexes: An IntroductionDocumento54 pagineSpinal Cord and Reflexes: An IntroductionLulu LuwiiNessuna valutazione finora
- 405 Genetics of DementiaDocumento12 pagine405 Genetics of DementiaLulu LuwiiNessuna valutazione finora
- Diagnosis and Treatment of Nystagmus PDFDocumento32 pagineDiagnosis and Treatment of Nystagmus PDFLulu LuwiiNessuna valutazione finora
- Close Finishnot Needed: DiagramDocumento2 pagineClose Finishnot Needed: DiagramLulu LuwiiNessuna valutazione finora
- A Workbook For Aphasia: Cleveland State UniversityDocumento116 pagineA Workbook For Aphasia: Cleveland State UniversityDesislava PeevaNessuna valutazione finora
- Crystalls & Mineralls MeaningsDocumento26 pagineCrystalls & Mineralls MeaningsCandice Cogburn100% (1)
- Antigens Antibodies and VaccinesDocumento4 pagineAntigens Antibodies and Vaccinesapi-299996815Nessuna valutazione finora
- Lesson 12 - Overview of The Wastewater Treatment ProcessDocumento6 pagineLesson 12 - Overview of The Wastewater Treatment ProcessZar ChiNessuna valutazione finora
- Measles Fact SheetDocumento1 paginaMeasles Fact Sheetapi-286128974Nessuna valutazione finora
- Acne Vulgaris PDFDocumento8 pagineAcne Vulgaris PDFsmackooooooNessuna valutazione finora
- College of Physicians and Surgeons of Ontario's Affidavit Re: Eve's Laser ClinicDocumento27 pagineCollege of Physicians and Surgeons of Ontario's Affidavit Re: Eve's Laser CliniccbcottawaNessuna valutazione finora
- Internet Gaming Disorder: A Case ReportDocumento4 pagineInternet Gaming Disorder: A Case ReportJAVED ATHER SIDDIQUINessuna valutazione finora
- Week 1 - Trauma (BB)Documento11 pagineWeek 1 - Trauma (BB)lizzy596Nessuna valutazione finora
- Cancer (Medical Term:Malignant NeoplasmDocumento7 pagineCancer (Medical Term:Malignant NeoplasmolussojiNessuna valutazione finora
- BODPUODocumento8 pagineBODPUOMiguel AradaNessuna valutazione finora
- Dre & Anoscopy: A Self-Directed Learning Module Clinical Skills Program Queen's UniversityDocumento10 pagineDre & Anoscopy: A Self-Directed Learning Module Clinical Skills Program Queen's UniversitymNessuna valutazione finora
- Therapy - Case Study 2Documento7 pagineTherapy - Case Study 2api-239581082100% (1)
- Tests That Will Elicit Cerebellar Signs Are inDocumento4 pagineTests That Will Elicit Cerebellar Signs Are inRaina DeWyzeNessuna valutazione finora
- Introduction To Pharmacokinetics: Deborah RobertsonDocumento3 pagineIntroduction To Pharmacokinetics: Deborah RobertsonTheresa Tyra SertaniNessuna valutazione finora
- Gut and Psychology Syndrome - Natural Treatment For Autism, Dyspraxia, A.D.130015Documento5 pagineGut and Psychology Syndrome - Natural Treatment For Autism, Dyspraxia, A.D.130015liza lizaNessuna valutazione finora
- Diabetic Ketoacidosis LODocumento19 pagineDiabetic Ketoacidosis LOlzbthshayNessuna valutazione finora
- Santos, Ivan Jamil S. NCM 112-Or Rle Fear (Pre-Op) Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocumento1 paginaSantos, Ivan Jamil S. NCM 112-Or Rle Fear (Pre-Op) Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveIvan SantosNessuna valutazione finora