Potrebbero piacerti anche
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- IABCanada AdGuidelines EnglishDocumento8 pagineIABCanada AdGuidelines EnglisheliasNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Datasheet: Intellitone™ Pro 200 Lan Toner and Probe SeriesDocumento5 pagineDatasheet: Intellitone™ Pro 200 Lan Toner and Probe SerieseliasNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- FMDocumento464 pagineFMeliasNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Final Cirrus PolDocumento4 pagineFinal Cirrus PoleliasNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Flyer InterPartyDialogue HighDocumento2 pagineFlyer InterPartyDialogue HigheliasNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Annual Report2017Documento47 pagineAnnual Report2017eliasNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Cougar Rock Campground: Mount Rainier National ParkDocumento1 paginaCougar Rock Campground: Mount Rainier National ParkeliasNessuna valutazione finora
- Fact Sheet The Career Developm 543255dbb3190Documento3 pagineFact Sheet The Career Developm 543255dbb3190eliasNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- A Study of The Canada-Korea Free Trade Negotiations: Lee Richardson, MP ChairDocumento54 pagineA Study of The Canada-Korea Free Trade Negotiations: Lee Richardson, MP ChaireliasNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Acado Matlab Manual PDFDocumento73 pagineAcado Matlab Manual PDFeliasNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- 08 2010 Mar Risk-Adjusted-continuousDocumento6 pagine08 2010 Mar Risk-Adjusted-continuouseliasNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The EU Strategy For Central Asia at Year One: Neil Melvin & Jos BoonstraDocumento10 pagineThe EU Strategy For Central Asia at Year One: Neil Melvin & Jos BoonstraeliasNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Keyback Key Facts: Important InformationDocumento2 pagineKeyback Key Facts: Important InformationeliasNessuna valutazione finora
- Guidance On Community Governance ReviewsDocumento53 pagineGuidance On Community Governance ReviewseliasNessuna valutazione finora
- Updated As of 2/5/2016Documento2 pagineUpdated As of 2/5/2016eliasNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- 2013CHI-Display Workshop EADocumento4 pagine2013CHI-Display Workshop EAeliasNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Duration of Regional Unemployment Spells in SloveniaDocumento24 pagineDuration of Regional Unemployment Spells in SloveniaeliasNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Unity and Diversity in Euro-Mediterranean Identities: Euro-European and Arabo-Mediterranean DimensionsDocumento14 pagineUnity and Diversity in Euro-Mediterranean Identities: Euro-European and Arabo-Mediterranean DimensionseliasNessuna valutazione finora
- Peran BF Dalam Pandemi Covid-VaksinDocumento28 paginePeran BF Dalam Pandemi Covid-VaksinFara EsterNessuna valutazione finora
- BCH2602 Bioenergetics Assignment 2 CompleteDocumento4 pagineBCH2602 Bioenergetics Assignment 2 CompleteNdumiso NdawondeNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
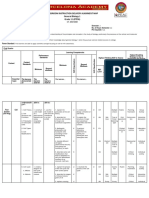
- Classroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)Documento6 pagineClassroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)JunedelMirallesPerez50% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Biology 1819 V2 Past PaperDocumento12 pagineBiology 1819 V2 Past PaperjcyNessuna valutazione finora
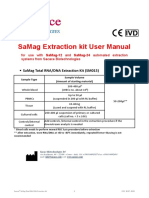
- 229f9 SaMag Total RNA-DNA Extraction Kit SM15 Ver 30072021Documento8 pagine229f9 SaMag Total RNA-DNA Extraction Kit SM15 Ver 30072021Danijel SelgradNessuna valutazione finora
- CHEM41290 Notes Part IDocumento25 pagineCHEM41290 Notes Part IJulia MachajNessuna valutazione finora
- Biochem COURSE SYLLABUSDocumento10 pagineBiochem COURSE SYLLABUSSharmaine DurangoNessuna valutazione finora
- Diagnostic Medical Microbiology Clinical CorrelationDocumento19 pagineDiagnostic Medical Microbiology Clinical CorrelationSaumya AnandNessuna valutazione finora
- HB-0405-005 HB RNY Plus 0920 WWDocumento48 pagineHB-0405-005 HB RNY Plus 0920 WWcffj6svp6nNessuna valutazione finora
- PCR Amplification assays-RAPD PDFDocumento5 paginePCR Amplification assays-RAPD PDFVedavyas DasariNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
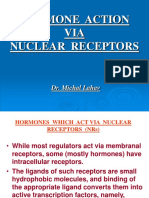
- Nuclear Receptors 2006Documento31 pagineNuclear Receptors 2006lsintaningtyasNessuna valutazione finora
- Syllabus Upload 2019 PDFDocumento55 pagineSyllabus Upload 2019 PDFMhohammad RifatNessuna valutazione finora
- Ashton Brennecke CV 2019Documento3 pagineAshton Brennecke CV 2019api-456822679Nessuna valutazione finora
- Lecture1 BIMM143 LargeDocumento73 pagineLecture1 BIMM143 Largepaseczkowo7Nessuna valutazione finora
- Advance Whitening Peptide Technology GenoWhite - 2017 SpainDocumento37 pagineAdvance Whitening Peptide Technology GenoWhite - 2017 SpainToni RosadiNessuna valutazione finora
- MEIOSISDocumento2 pagineMEIOSISKim BeatrizNessuna valutazione finora
- Ranbaxy Laboratories LimitedDocumento9 pagineRanbaxy Laboratories LimitedNeerajNessuna valutazione finora
- Overview of Post-Translational Modification AnalysisDocumento2 pagineOverview of Post-Translational Modification AnalysisSteven4654Nessuna valutazione finora
- June 2019 QP - Paper 1 B Edexcel Biology IGCSEDocumento32 pagineJune 2019 QP - Paper 1 B Edexcel Biology IGCSEhassanNessuna valutazione finora
- Molecular Biology FundamentalDocumento26 pagineMolecular Biology FundamentalSoporte general IT1Nessuna valutazione finora
- Novavax Initiates COVID-19 Vaccine Clinical Trial CrossoverDocumento2 pagineNovavax Initiates COVID-19 Vaccine Clinical Trial CrossoverDavid SantosNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- ICFRE Scientist Recruitment 18feb10Documento9 pagineICFRE Scientist Recruitment 18feb10cvrcmrNessuna valutazione finora
- Blue Print PB-2 Class 12 BioDocumento2 pagineBlue Print PB-2 Class 12 Biopranjalbhardwaj11Nessuna valutazione finora
- Combinatorial Chemistry Amp High Throughput Screening PDFDocumento2 pagineCombinatorial Chemistry Amp High Throughput Screening PDFLamarcusNessuna valutazione finora
- Industrial Training Report - UniklDocumento29 pagineIndustrial Training Report - Uniklzul100% (3)
- Numbers Sheet Name Numbers Table Name Excel Worksheet NameDocumento5 pagineNumbers Sheet Name Numbers Table Name Excel Worksheet Namecrm testNessuna valutazione finora
- Bản Dịch Của Tài Liệu Không Có Tiêu ĐềDocumento13 pagineBản Dịch Của Tài Liệu Không Có Tiêu Đềbao739601Nessuna valutazione finora
- Promega HaloTag Fusion Protein GuideDocumento3 paginePromega HaloTag Fusion Protein GuideMoritz ListNessuna valutazione finora
- LAS 4 Science 9 QRT 1 Week 4 RTP FinalDocumento4 pagineLAS 4 Science 9 QRT 1 Week 4 RTP FinalSunday MochicanaNessuna valutazione finora
- Mitosis Vs Meiosis ReadingDocumento3 pagineMitosis Vs Meiosis Readingshazia imamNessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (4)