Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Smart Science 6Documento16 pagineSmart Science 6april light67% (3)
- Crochet Pattern For A Human Heart: Valérie Prieur-Côté May 3, 2018Documento7 pagineCrochet Pattern For A Human Heart: Valérie Prieur-Côté May 3, 2018Ale ReséndizNessuna valutazione finora
- Life Processes Class 10 Notes Biolog1Documento8 pagineLife Processes Class 10 Notes Biolog1Eashurock KnigamNessuna valutazione finora
- CH 19 Transport in HumanDocumento49 pagineCH 19 Transport in HumanRay PeramathevanNessuna valutazione finora
- USABO 18 Open Exam - Final Wo AnsDocumento17 pagineUSABO 18 Open Exam - Final Wo AnsJ.Chang ChangNessuna valutazione finora
- Open Heart SurgeriesDocumento48 pagineOpen Heart SurgeriesHoney PrasadNessuna valutazione finora
- 2 Phlebotomy Notes Taken From The Lecture of Sir Antonio Pascua JR RMTDocumento5 pagine2 Phlebotomy Notes Taken From The Lecture of Sir Antonio Pascua JR RMTRhoda Mae CubillaNessuna valutazione finora
- American Academy of Aesthetic Medicine Level 1Documento11 pagineAmerican Academy of Aesthetic Medicine Level 1Lydia KirbyNessuna valutazione finora
- Dermatology MCQ 1700Documento45 pagineDermatology MCQ 1700Dr-Jahanzaib Gondal100% (1)
- Principles of Patient PositioningDocumento62 paginePrinciples of Patient PositioningMelody JusticeNessuna valutazione finora
- ULAM, CHIN V. - NCM 118 PrelimDocumento8 pagineULAM, CHIN V. - NCM 118 PrelimChin Villanueva Ulam100% (1)
- Cover LetterDocumento1 paginaCover LetterdnazaryNessuna valutazione finora
- Galley ProofDocumento4 pagineGalley ProofdnazaryNessuna valutazione finora
- ReferensiDocumento3 pagineReferensidnazaryNessuna valutazione finora
- Oi2011 PDFDocumento8 pagineOi2011 PDFdnazaryNessuna valutazione finora
- Title PageDocumento1 paginaTitle PagednazaryNessuna valutazione finora
- Nocun2015 PDFDocumento5 pagineNocun2015 PDFdnazaryNessuna valutazione finora
- Endoscopic Ventriculostomy Versus Shunt Operation in Normal Pressure Hydrocephalus: Diagnostics and IndicationDocumento4 pagineEndoscopic Ventriculostomy Versus Shunt Operation in Normal Pressure Hydrocephalus: Diagnostics and IndicationdnazaryNessuna valutazione finora
- Effects of Information Provision Activities in Streets On Driving SpeedsDocumento8 pagineEffects of Information Provision Activities in Streets On Driving SpeedsdnazaryNessuna valutazione finora
- Cornell A 2003Documento13 pagineCornell A 2003dnazaryNessuna valutazione finora
- T S M P H: HE Urgical Anagement of Ediatric YdrocephalusDocumento10 pagineT S M P H: HE Urgical Anagement of Ediatric YdrocephalusdnazaryNessuna valutazione finora
- Berg Sneider 2008Documento18 pagineBerg Sneider 2008dnazaryNessuna valutazione finora
- Diagnosis and Management of Idiopathic Normal-Pressure HydrocephalusDocumento11 pagineDiagnosis and Management of Idiopathic Normal-Pressure HydrocephalusdnazaryNessuna valutazione finora
- Hemifacial Spasm A NeurosurgicalDocumento8 pagineHemifacial Spasm A NeurosurgicaldnazaryNessuna valutazione finora
- Treatment of Hydrocephalus: Mere Survival Is Not EnoughDocumento7 pagineTreatment of Hydrocephalus: Mere Survival Is Not EnoughdnazaryNessuna valutazione finora
- Tests General 08Documento32 pagineTests General 08melvingeorge200950% (2)
- Joukal (2017) Anatomy of The Human Visual PathwayDocumento16 pagineJoukal (2017) Anatomy of The Human Visual PathwaysektemujibNessuna valutazione finora
- Learning Resource Workbook Science 6-Analyn Gaballo PagsabanganDocumento6 pagineLearning Resource Workbook Science 6-Analyn Gaballo PagsabanganJohana BALASNessuna valutazione finora
- Abbreviations 2011Documento27 pagineAbbreviations 2011Takahito KamimuraNessuna valutazione finora
- Hemodynamic DisordersDocumento6 pagineHemodynamic DisordersPradeep100% (1)
- 2012-03 - Resection of Tumors of The Neck of The Pancreas With Venous Invasion - The "Whipple at The Splenic Artery (WATSA) " Procedure PDFDocumento7 pagine2012-03 - Resection of Tumors of The Neck of The Pancreas With Venous Invasion - The "Whipple at The Splenic Artery (WATSA) " Procedure PDFNawzad SulayvaniNessuna valutazione finora
- Deep Vein Thrombosis FlyerDocumento2 pagineDeep Vein Thrombosis FlyerMuhammad Reza Syahli PiliangNessuna valutazione finora
- Dog Heart (Plastinated)Documento3 pagineDog Heart (Plastinated)Roger CallNessuna valutazione finora
- Pelvic ThrombophlebitisDocumento12 paginePelvic ThrombophlebitisMicah Magallano100% (1)
- AVBS2001Documento81 pagineAVBS2001Celine Berjot100% (1)
- The Hazards: OF Blood TransfusionDocumento7 pagineThe Hazards: OF Blood TransfusionPranjal Kr SahariaNessuna valutazione finora
- Guia Esvs Manejo Evc 2015Documento60 pagineGuia Esvs Manejo Evc 2015Steeven Ruilova Valle100% (1)
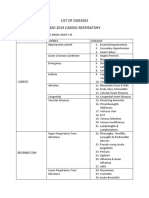
- List of Diseases Imo 2019 Cardio-RespiratoryDocumento2 pagineList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNessuna valutazione finora
- CVS MonitoringDocumento33 pagineCVS MonitoringMicheal NorrisNessuna valutazione finora
- Med Term Study GuideDocumento706 pagineMed Term Study GuideJesse LeonardNessuna valutazione finora
- Anesthesia For Maxillofacial ProcedureDocumento90 pagineAnesthesia For Maxillofacial ProcedureShalini Thakur Dubey0% (2)
- Systemic CirculationDocumento3 pagineSystemic CirculationWira SentanuNessuna valutazione finora
- TV MCQ Pertanyaan TokDocumento5 pagineTV MCQ Pertanyaan TokdhinahafizNessuna valutazione finora
- Science - G9 - Week 2 (Lessons-4-6)Documento46 pagineScience - G9 - Week 2 (Lessons-4-6)Rhyan Zero-four BaluyutNessuna valutazione finora