Potrebbero piacerti anche
- BDSM Checklist ShevahDocumento208 pagineBDSM Checklist Shevahslackjack86% (36)
- Mount and Blade Warband RGL ConfigDocumento3 pagineMount and Blade Warband RGL ConfigShelby WhitfieldNessuna valutazione finora
- Schedule of Rates 2011 Rev1Documento144 pagineSchedule of Rates 2011 Rev1Screen BiruNessuna valutazione finora
- DOE Description & Picture List Price 2020 PDFDocumento127 pagineDOE Description & Picture List Price 2020 PDFNizam AmirNessuna valutazione finora
- Comparison Shear Wall and Brick WallDocumento15 pagineComparison Shear Wall and Brick Wallnawazkhan23Nessuna valutazione finora
- Guard HouseDocumento2 pagineGuard HouseKevin LowNessuna valutazione finora
- Civil Engeneering, Steel Structure Building, Interior, Mecanichal, Electrical Stainless Steel and PipingDocumento6 pagineCivil Engeneering, Steel Structure Building, Interior, Mecanichal, Electrical Stainless Steel and Pipingkrisna kingNessuna valutazione finora
- Lembaga Arkitek Malaysia (Lam) Inspector of Work (Iow) Practical Experience Log Book GuideDocumento7 pagineLembaga Arkitek Malaysia (Lam) Inspector of Work (Iow) Practical Experience Log Book GuideMuhammad Zulfadhli0% (1)
- SCAE MT 4040 Traffic Light Controller Spare PartsDocumento3 pagineSCAE MT 4040 Traffic Light Controller Spare Partsleong2007Nessuna valutazione finora
- Nisbah Konkrit g40Documento3 pagineNisbah Konkrit g40Faeez ZainNessuna valutazione finora
- Hydroponics - Introduction To HydroponicsDocumento91 pagineHydroponics - Introduction To HydroponicscorradiniaNessuna valutazione finora
- Hemorrhagic Stroke CBLDocumento106 pagineHemorrhagic Stroke CBLJessica NadiaNessuna valutazione finora
- Aoun, Lucas (2021) BOOST YOUR BRAIN - A Beginner's Guide To Leverage The Power of Nootropics For Ultimate Brain EnhancementDocumento49 pagineAoun, Lucas (2021) BOOST YOUR BRAIN - A Beginner's Guide To Leverage The Power of Nootropics For Ultimate Brain EnhancementJordan67% (3)
- Seminar On Standardising and Enhancing Bills of Quantities For Civil Engineering Works Using Malaysian Standard Method of Measurement (Cesmm)Documento38 pagineSeminar On Standardising and Enhancing Bills of Quantities For Civil Engineering Works Using Malaysian Standard Method of Measurement (Cesmm)Nurhayati Muhamad Nor100% (1)
- Modern Agro Project ReportDocumento47 pagineModern Agro Project ReportCik Sri Syarifah100% (1)
- Sample Civil BoqDocumento57 pagineSample Civil Boqkvamshi_1971Nessuna valutazione finora
- Sewerage (All Provisional) Sewer PipeDocumento6 pagineSewerage (All Provisional) Sewer Pipenur shafiqahNessuna valutazione finora
- ECOSEPT P-Series CatalogueDocumento2 pagineECOSEPT P-Series Catalogueaniza zazaNessuna valutazione finora
- STORAGE TANK SPECIFICATIONSDocumento1 paginaSTORAGE TANK SPECIFICATIONSMohamed ZaihasrenNessuna valutazione finora
- Section L - Water Reticulation, Internal Plumbing System and Sanitary FittingsDocumento14 pagineSection L - Water Reticulation, Internal Plumbing System and Sanitary FittingsMahadhir MohammadNessuna valutazione finora
- Anti termite treatment for staff quarters projectDocumento2 pagineAnti termite treatment for staff quarters projectfasihaNessuna valutazione finora
- API - A Specialist in Precast Concrete ProductsDocumento3 pagineAPI - A Specialist in Precast Concrete Productsalgebra1975100% (1)
- JKR Standard Specification 2014Documento1 paginaJKR Standard Specification 2014Mohd Izzuddin ZainiNessuna valutazione finora
- Specification For Suppliers PDFDocumento7 pagineSpecification For Suppliers PDFalep azizNessuna valutazione finora
- JKH 2019 JpediaDocumento50 pagineJKH 2019 JpediaAsmaa AthirahNessuna valutazione finora
- Borang ProbaDocumento2 pagineBorang Proba290902100% (1)
- Borang Mackintosh ProbeDocumento2 pagineBorang Mackintosh ProbezamzuraneeNessuna valutazione finora
- JKR 20401Documento8 pagineJKR 20401dinu69inNessuna valutazione finora
- Method Statement For Mackintosh Probe TestDocumento1 paginaMethod Statement For Mackintosh Probe TestNurLiyana RasmiNessuna valutazione finora
- Take Into Account These Losses When Purchasing Power Transformer - EEPDocumento7 pagineTake Into Account These Losses When Purchasing Power Transformer - EEPAbdul Mohid SheikhNessuna valutazione finora
- Fencing PriceDocumento2 pagineFencing PriceAana SamsNessuna valutazione finora
- BQ PmuDocumento5 pagineBQ PmuAzamOthman100% (1)
- Report Futsal Court KemasekDocumento24 pagineReport Futsal Court Kemasekaldeto71Nessuna valutazione finora
- BAB 4 (B) CompactionDocumento6 pagineBAB 4 (B) Compactionabood buriahiNessuna valutazione finora
- Pembekal Kekuda Bumbung PDFDocumento15 paginePembekal Kekuda Bumbung PDFhanif100% (1)
- Q12895Z-Hospital Serdang-FCUs PDFDocumento1 paginaQ12895Z-Hospital Serdang-FCUs PDFsueNessuna valutazione finora
- Borang K-2Documento4 pagineBorang K-2Azuanuddin Samad100% (1)
- (Bedroom 1 Measurement of First Floor Internal WallsDocumento26 pagine(Bedroom 1 Measurement of First Floor Internal Wallswilliam khooNessuna valutazione finora
- Bill of Quantities: IndexDocumento42 pagineBill of Quantities: IndexLe JennieNessuna valutazione finora
- R&D ContohDocumento26 pagineR&D ContohfeedNessuna valutazione finora
- G2 FinalreportDocumento219 pagineG2 Finalreportazhar ahmadNessuna valutazione finora
- Lab EquipmentDocumento3 pagineLab Equipmentemily storyNessuna valutazione finora
- Phraseology Bils of Quantity (For Academic Purposes Only) 2009Documento169 paginePhraseology Bils of Quantity (For Academic Purposes Only) 2009diana anuarNessuna valutazione finora
- Application of Braced and Unbraced Frame in Reinforced Concrete StructureDocumento2 pagineApplication of Braced and Unbraced Frame in Reinforced Concrete StructureNazmi DhiyauddinNessuna valutazione finora
- Unit QTY Rate Amount Rate RefDocumento9 pagineUnit QTY Rate Amount Rate RefC.SnojanNessuna valutazione finora
- Precast Concrete Pile RatesDocumento5 paginePrecast Concrete Pile RatesAbdulrani AbuNessuna valutazione finora
- Analyzing concrete strength for a mosque construction projectDocumento2 pagineAnalyzing concrete strength for a mosque construction projectSuper Awesome PersonNessuna valutazione finora
- Preliminary Cost Estimate for Proposed BuildingDocumento3 paginePreliminary Cost Estimate for Proposed BuildingAdib HilmanNessuna valutazione finora
- Revison Ques CH 2Documento6 pagineRevison Ques CH 2hildaNessuna valutazione finora
- PipeworksDocumento5 paginePipeworksNurulSyarinaAlyaNessuna valutazione finora
- Method Statement Pipe JackingDocumento1 paginaMethod Statement Pipe JackingNur NeynaNessuna valutazione finora
- Standard Specification: Section 8: Traffic Signal SystemDocumento7 pagineStandard Specification: Section 8: Traffic Signal SystemMohd Izzuddin ZainiNessuna valutazione finora
- Week 3 - CIVE 4703 (WBLFF)Documento12 pagineWeek 3 - CIVE 4703 (WBLFF)nicholasNessuna valutazione finora
- Fees for water services infrastructure planning and designDocumento1 paginaFees for water services infrastructure planning and designJohnyReubenNessuna valutazione finora
- Preambles to All TradesDocumento12 paginePreambles to All TradesMohamad Noor AffenddyNessuna valutazione finora
- Class F ContractorDocumento23 pagineClass F ContractorRachel IngramNessuna valutazione finora
- Training & Experience Report (Outcome-Based PAE)Documento8 pagineTraining & Experience Report (Outcome-Based PAE)Hafizul AminNessuna valutazione finora
- Harga Purata Simen Di Semenanjung Malaysia, Sabah Dan Sarawak Bagi Tahun 2014 Hingga 2017Documento2 pagineHarga Purata Simen Di Semenanjung Malaysia, Sabah Dan Sarawak Bagi Tahun 2014 Hingga 2017sanglimNessuna valutazione finora
- Guidelines KL Bike Pedestrian 2019 2028Documento88 pagineGuidelines KL Bike Pedestrian 2019 2028saraseeraNessuna valutazione finora
- EAT 250 Esteem Software TutorialDocumento25 pagineEAT 250 Esteem Software TutorialsofiyanasirNessuna valutazione finora
- Signature of Owner: Borang PDC 2Documento8 pagineSignature of Owner: Borang PDC 2Mageswary KunalanNessuna valutazione finora
- Project Evaluation and DevelopmentDocumento158 pagineProject Evaluation and DevelopmentRosbella Rohaizar100% (1)
- The Conditions For Water Reticulation Plans-Part2Documento1 paginaThe Conditions For Water Reticulation Plans-Part2edwinhlcNessuna valutazione finora
- Medical Form 24.10.2023Documento1 paginaMedical Form 24.10.2023gdspriyadarshana84Nessuna valutazione finora
- Medical ReportDocumento5 pagineMedical ReportXYZNessuna valutazione finora
- Estimates and Sample Size With One Sample: © The Mcgraw-Hill Companies, Inc., 2000Documento29 pagineEstimates and Sample Size With One Sample: © The Mcgraw-Hill Companies, Inc., 2000Wilson LimNessuna valutazione finora
- Chapter 4 Second Order DEsDocumento59 pagineChapter 4 Second Order DEsfifafifaNessuna valutazione finora
- Project MilestoneDocumento2 pagineProject MilestoneWilson LimNessuna valutazione finora
- Transfer Function - by AnalogyDocumento22 pagineTransfer Function - by AnalogyMohd Ridzuan AhmadNessuna valutazione finora
- DDocumento7 pagineDWilson LimNessuna valutazione finora
- Gas Power Cycles - Part 2 - KamalDocumento54 pagineGas Power Cycles - Part 2 - KamalWilson LimNessuna valutazione finora
- Mechanics of Machines Belt Drive SystemDocumento58 pagineMechanics of Machines Belt Drive SystemWilson Lim100% (1)
- Bda 2033 Chapter 1-Gear SystemDocumento27 pagineBda 2033 Chapter 1-Gear SystemWilson LimNessuna valutazione finora
- Mechanics of Machines Belt Drive SystemDocumento58 pagineMechanics of Machines Belt Drive SystemWilson Lim100% (1)
- Universal Coupling Lab Static Dynamic PDFDocumento4 pagineUniversal Coupling Lab Static Dynamic PDFWilson Lim0% (1)
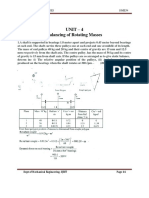
- Unit - 4 Balancing of Rotating Masses: A C T Ss Fe Spe T Vely Ce y S - , e e (I I GsDocumento8 pagineUnit - 4 Balancing of Rotating Masses: A C T Ss Fe Spe T Vely Ce y S - , e e (I I GsKong DuiDuiNessuna valutazione finora
- Fluid Foc2Documento2 pagineFluid Foc2Wilson LimNessuna valutazione finora
- Project Solid 2Documento1 paginaProject Solid 2Wilson LimNessuna valutazione finora
- Theory and ConclDocumento2 pagineTheory and ConclWilson LimNessuna valutazione finora
- Gear SystemDocumento57 pagineGear SystemWilson LimNessuna valutazione finora
- Universal Coupling Lab Static Dynamic PDFDocumento4 pagineUniversal Coupling Lab Static Dynamic PDFWilson Lim0% (1)
- Serial KeyDocumento1 paginaSerial KeyWilson LimNessuna valutazione finora
- Wave Equations SolverDocumento14 pagineWave Equations SolverWilson LimNessuna valutazione finora
- Creative Problem Solving: An OverviewDocumento14 pagineCreative Problem Solving: An OverviewWilson LimNessuna valutazione finora
- Rubber eDocumento16 pagineRubber eWilson LimNessuna valutazione finora
- Fluid Dynamics CharacteristicsDocumento50 pagineFluid Dynamics CharacteristicsWilson LimNessuna valutazione finora
- Water Level Indicator Project ReportDocumento9 pagineWater Level Indicator Project ReportManoj PatilNessuna valutazione finora
- c6 Problem StatementDocumento13 paginec6 Problem StatementWilson LimNessuna valutazione finora
- Creativity AND Innovation: Problem DefinitionDocumento7 pagineCreativity AND Innovation: Problem DefinitionWilson LimNessuna valutazione finora
- C5 Data GatheringDocumento13 pagineC5 Data GatheringWilson LimNessuna valutazione finora
- 04ns LaplaceDocumento11 pagine04ns LaplaceAfiq NaqiuddinNessuna valutazione finora
- DDocumento7 pagineDWilson LimNessuna valutazione finora
- OSH strategies to improve workplace safetyDocumento3 pagineOSH strategies to improve workplace safetyWilson LimNessuna valutazione finora
- Fascinating Facts About the Human Body and BeyondDocumento3 pagineFascinating Facts About the Human Body and BeyondWilson LimNessuna valutazione finora
- Dickens and Bio Politics. ArticleDocumento24 pagineDickens and Bio Politics. ArticleJose Luis FernandezNessuna valutazione finora
- 150 Agribusiness Ideas For 2018Documento40 pagine150 Agribusiness Ideas For 2018Laurent AnabaNessuna valutazione finora
- Pregnancy Nursing Diagnosis and Care PlanDocumento12 paginePregnancy Nursing Diagnosis and Care PlanJeane Louise PalmeroNessuna valutazione finora
- 11 Oxirane GC MSDocumento6 pagine11 Oxirane GC MSCHRISTIAN FELIPE JIMENEZ MURILLONessuna valutazione finora
- Electrochemical Methods For The Analysis of Clinically RelevantDocumento90 pagineElectrochemical Methods For The Analysis of Clinically Relevantch_ymyaaNessuna valutazione finora
- No Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanDocumento16 pagineNo Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanNurmalasari SaryNessuna valutazione finora
- Samadhan 1 - MergedDocumento109 pagineSamadhan 1 - MergedPranjal Raj SinghNessuna valutazione finora
- Peran Perawat Pada Pemeriksaan Penunjang IVUS, OCT (Imaging)Documento31 paginePeran Perawat Pada Pemeriksaan Penunjang IVUS, OCT (Imaging)Miftahul HudaNessuna valutazione finora
- Physical and Mental Health of The Workers in The Readymade Garment Industry of BangladeshDocumento10 paginePhysical and Mental Health of The Workers in The Readymade Garment Industry of BangladeshDr. Nazrul IslamNessuna valutazione finora
- Biosimilars JapanDocumento2 pagineBiosimilars JapanVijay Nag ThotaNessuna valutazione finora
- Adolescence Personality TheoryDocumento9 pagineAdolescence Personality TheoryEyn Herrera Granatin100% (1)
- Sop For Periodic FitnessDocumento6 pagineSop For Periodic FitnessEkum EdunghuNessuna valutazione finora
- Build A Virus Lesson Plan 2 20 12Documento8 pagineBuild A Virus Lesson Plan 2 20 12M9094Nessuna valutazione finora
- VERVE DYNAMICS - African Dream and Other Gels - 2017Documento4 pagineVERVE DYNAMICS - African Dream and Other Gels - 2017Lesley HollardNessuna valutazione finora
- Gastro Intestinal Tract: Dr. Indu MandalDocumento18 pagineGastro Intestinal Tract: Dr. Indu Mandalankit ahirNessuna valutazione finora
- Carbohydrates Clinical SignificanceDocumento10 pagineCarbohydrates Clinical SignificanceMay Ann EnoserioNessuna valutazione finora
- Nurs 3020 - Erin Final EvaluationDocumento14 pagineNurs 3020 - Erin Final Evaluationapi-505854426Nessuna valutazione finora
- Ipdoaj MS Id 000113Documento3 pagineIpdoaj MS Id 000113Ayu DamayNessuna valutazione finora
- Emergency and Disaster NursingDocumento13 pagineEmergency and Disaster Nursingkarenkaren09Nessuna valutazione finora
- The Positive Effects of Tourism With Horse Riding On Human Health - C. Yıldırım, H. Çalışkan, M. T. Koçkar, A. E. Ün, M. Ünlüoğlu, 2018Documento15 pagineThe Positive Effects of Tourism With Horse Riding On Human Health - C. Yıldırım, H. Çalışkan, M. T. Koçkar, A. E. Ün, M. Ünlüoğlu, 2018M. Tekin KOÇKARNessuna valutazione finora
- Script For Head To NeckDocumento7 pagineScript For Head To NeckSydney Joy Abaca100% (1)
- Daftar Pustaka KorneaDocumento3 pagineDaftar Pustaka KorneaMuhammad Apriliandy ShariffNessuna valutazione finora
- Test Bank For Health Psychology 3rd Edition SandersonDocumento10 pagineTest Bank For Health Psychology 3rd Edition SandersonpudgyoverburnnggNessuna valutazione finora
- Investigation of Blood Culture Using BACTEC SystemsDocumento36 pagineInvestigation of Blood Culture Using BACTEC SystemsGregorio De Las CasasNessuna valutazione finora
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDocumento8 pagineVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengNessuna valutazione finora