Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- SLE Made EasyDocumento482 pagineSLE Made EasySumayyia Qamar100% (1)
- Sickle Cell AnemiaDocumento63 pagineSickle Cell Anemiaoss-20502745100% (4)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Id No.: CVD/NCD Assessment Form For Adults 20 Years Old and AboveDocumento1 paginaId No.: CVD/NCD Assessment Form For Adults 20 Years Old and AboveNel Jerez67% (3)
- KneeDocumento14 pagineKneeJohnpeter Esporlas100% (1)
- Frequency DR Hulda Clark ZapperDocumento45 pagineFrequency DR Hulda Clark ZapperkwbutterfliesNessuna valutazione finora
- CVA Bleed vs. InfarctDocumento33 pagineCVA Bleed vs. InfarctPaul Henry RoxasNessuna valutazione finora
- Mes 3Documento4 pagineMes 3Johnpeter EsporlasNessuna valutazione finora
- MOSCO'S CLERKING GUIDEDocumento88 pagineMOSCO'S CLERKING GUIDEtemitopeNessuna valutazione finora
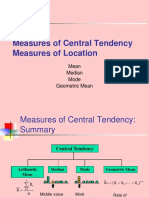
- Central TendencyDocumento25 pagineCentral TendencyJohnpeter EsporlasNessuna valutazione finora
- Amyotrophic Lateral SclerosisDocumento3 pagineAmyotrophic Lateral SclerosisJohnpeter EsporlasNessuna valutazione finora
- CBR Topic Outline 2017-2018Documento3 pagineCBR Topic Outline 2017-2018Johnpeter EsporlasNessuna valutazione finora
- Renr Practice Test 9 FinalDocumento12 pagineRenr Practice Test 9 FinalTk100% (2)
- Assistive Devices RealDocumento3 pagineAssistive Devices RealJohnpeter EsporlasNessuna valutazione finora
- B. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactDocumento4 pagineB. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactJohnpeter EsporlasNessuna valutazione finora
- Achalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionDocumento10 pagineAchalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionJohnpeter EsporlasNessuna valutazione finora
- Is There Anything Left to Trust? - 40-character for document on trusting the BibleDocumento28 pagineIs There Anything Left to Trust? - 40-character for document on trusting the BibleJohnpeter EsporlasNessuna valutazione finora
- Introduction To PharmacologyDocumento6 pagineIntroduction To PharmacologyJohnpeter EsporlasNessuna valutazione finora
- Bell's PalsyDocumento9 pagineBell's PalsyJohnpeter EsporlasNessuna valutazione finora
- Parables of Jesus ChristDocumento4 pagineParables of Jesus ChristJohnpeter EsporlasNessuna valutazione finora
- Pediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageDocumento3 paginePediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageJohnpeter EsporlasNessuna valutazione finora
- Postpolio SyndromeDocumento3 paginePostpolio SyndromeJohnpeter Esporlas100% (1)
- ReviewDocumento10 pagineReviewJohnpeter EsporlasNessuna valutazione finora
- Electrotherapy Parameters For Grand PraxDocumento3 pagineElectrotherapy Parameters For Grand PraxJohnpeter EsporlasNessuna valutazione finora
- TEP 2 Syllabus and Course Overviews for Physiotherapy ModulesDocumento2 pagineTEP 2 Syllabus and Course Overviews for Physiotherapy ModulesJohnpeter EsporlasNessuna valutazione finora
- Chapter 12Documento22 pagineChapter 12John EmmanuelNessuna valutazione finora
- Down SyndromeDocumento2 pagineDown SyndromeJohnpeter EsporlasNessuna valutazione finora
- Tep 11 Reflexes PrintoutDocumento2 pagineTep 11 Reflexes PrintoutJohnpeter EsporlasNessuna valutazione finora
- Effects of Prolonged Immobilization on the Musculoskeletal SystemDocumento14 pagineEffects of Prolonged Immobilization on the Musculoskeletal SystemJohnpeter EsporlasNessuna valutazione finora
- Patient Survey Results Guide Practice ImprovementsDocumento6 paginePatient Survey Results Guide Practice ImprovementsJohnpeter EsporlasNessuna valutazione finora
- Cardiovascular RehabilitationDocumento5 pagineCardiovascular RehabilitationJohnpeter EsporlasNessuna valutazione finora
- Normal Body TemperaturesDocumento5 pagineNormal Body TemperaturesJohnpeter EsporlasNessuna valutazione finora
- SHOULDER PAIN AND INJURY GUIDEDocumento7 pagineSHOULDER PAIN AND INJURY GUIDEJohnpeter EsporlasNessuna valutazione finora
- Neuroanatomy Pictures Part 2 - WaxmanDocumento6 pagineNeuroanatomy Pictures Part 2 - WaxmanJohnpeter EsporlasNessuna valutazione finora
- Atlas of Digestive SystemDocumento3 pagineAtlas of Digestive SystemJohnpeter EsporlasNessuna valutazione finora
- Anthropometric SDocumento3 pagineAnthropometric SJohnpeter EsporlasNessuna valutazione finora
- Etiology, Epidemiology & Differential Diagnosis For CADDocumento9 pagineEtiology, Epidemiology & Differential Diagnosis For CADJohnpeter EsporlasNessuna valutazione finora
- 40 - Advances in Motion and Electromyography Based Wearabletechnology For Upper Extremity Function Rehabilitation A ReviewDocumento7 pagine40 - Advances in Motion and Electromyography Based Wearabletechnology For Upper Extremity Function Rehabilitation A Reviewmihaela_986230018Nessuna valutazione finora
- Medical Questionnaire For PatientsDocumento1 paginaMedical Questionnaire For Patientsjrepko1Nessuna valutazione finora
- Prevalence and Impact of Pain Among Older Adults in The United StatesDocumento9 paginePrevalence and Impact of Pain Among Older Adults in The United StatesLucas TarquiNessuna valutazione finora
- Saxion Physiotherapy Curriculum OverviewDocumento22 pagineSaxion Physiotherapy Curriculum OverviewGretel EdelweissNessuna valutazione finora
- Healthmedicinet I 2017 5Documento630 pagineHealthmedicinet I 2017 5tuni santeNessuna valutazione finora
- Treatment of Upper Extremity Spasticity in Stroke Patients by Focal Neuronal or Neuromuscular Blockade: A Systematic Review of The LiteratureDocumento11 pagineTreatment of Upper Extremity Spasticity in Stroke Patients by Focal Neuronal or Neuromuscular Blockade: A Systematic Review of The LiteraturemitroisergiuNessuna valutazione finora
- Contoh Soal KMB Ujikom 1Documento34 pagineContoh Soal KMB Ujikom 1RobbyNessuna valutazione finora
- Overview of Primary Prevention of Coronary Heart Disease and Stroke - UpToDateDocumento15 pagineOverview of Primary Prevention of Coronary Heart Disease and Stroke - UpToDatethanh phung phamNessuna valutazione finora
- DynaMed Plus - Stroke (Acute Management)Documento126 pagineDynaMed Plus - Stroke (Acute Management)Sarah Shafa MarwadhaniNessuna valutazione finora
- Hubungan Gerd Dengan DepresiDocumento8 pagineHubungan Gerd Dengan DepresiDella Elvina RoeslandNessuna valutazione finora
- Padillo Vs Rural BankDocumento6 paginePadillo Vs Rural BankheymissrubyNessuna valutazione finora
- Stroke Incidence and Case Fatality in AustralasiaDocumento7 pagineStroke Incidence and Case Fatality in AustralasiaChintya Anugrah SuhendraNessuna valutazione finora
- European Stroke ScaleDocumento3 pagineEuropean Stroke ScaleAbdur RasyidNessuna valutazione finora
- 328 IndexDocumento29 pagine328 IndexDafi SanNessuna valutazione finora
- Comparison of CT and MR Imaging in Ischemic StrokeDocumento10 pagineComparison of CT and MR Imaging in Ischemic Strokeتغريد عبادةNessuna valutazione finora
- Neuromuscular Therapy Techniques for Stroke and MS RehabilitationDocumento11 pagineNeuromuscular Therapy Techniques for Stroke and MS RehabilitationWenzy Razzie cruzNessuna valutazione finora
- Shep TrialDocumento10 pagineShep TrialOlayemi OladiranNessuna valutazione finora
- Ezetimibe Added To Statin Therapy After Acute Coronary SyndromesDocumento11 pagineEzetimibe Added To Statin Therapy After Acute Coronary SyndromesAngela DelarmenteNessuna valutazione finora
- Ijms 13 11753 PDFDocumento20 pagineIjms 13 11753 PDFVandy IkraNessuna valutazione finora
- Advances in Intracranial HemorrhageDocumento15 pagineAdvances in Intracranial HemorrhageJorge GonzalesNessuna valutazione finora
- Impact of High Altitude On Cardiovascular Health: Current PerspectivesDocumento19 pagineImpact of High Altitude On Cardiovascular Health: Current PerspectivesveronicaNessuna valutazione finora
- 16 Vascular Diseases of Nervous System-QDocumento24 pagine16 Vascular Diseases of Nervous System-QAdi PomeranzNessuna valutazione finora
- Secure your family's future with this adjustable life insurance planDocumento25 pagineSecure your family's future with this adjustable life insurance planaaaNessuna valutazione finora