Potrebbero piacerti anche
- DIAGNOSING HYPERTENSION: BLOOD PRESSURE MEASUREMENT GUIDEDocumento37 pagineDIAGNOSING HYPERTENSION: BLOOD PRESSURE MEASUREMENT GUIDEDhira 'Princess Kalonk' AninditaNessuna valutazione finora
- How To Measure BPDocumento25 pagineHow To Measure BPSenen PaezNessuna valutazione finora
- Agustus Monitoring HemodinamikDocumento61 pagineAgustus Monitoring HemodinamikFikriYTNessuna valutazione finora
- Assessing Volume StatusDocumento12 pagineAssessing Volume StatusMoises Torres AlvarezNessuna valutazione finora
- Racial Bias in Pulse Oximetry Measurement: CorrespondenceDocumento2 pagineRacial Bias in Pulse Oximetry Measurement: CorrespondenceYony Gutierrez100% (1)
- Baska MaskDocumento8 pagineBaska MaskAnish H DaveNessuna valutazione finora
- Piccolo Xpress Chemistry Analyser SOPDocumento16 paginePiccolo Xpress Chemistry Analyser SOPBahamas Wellness Diagnostic ServicesNessuna valutazione finora
- Invasive Blood Pressure Monitoring - Technical ConsiderationDocumento29 pagineInvasive Blood Pressure Monitoring - Technical ConsiderationubaidrahamanNessuna valutazione finora
- Hemodynamic MonitoringDocumento23 pagineHemodynamic MonitoringIrvan SetiawanNessuna valutazione finora
- ICP AlgorithmDocumento1 paginaICP AlgorithmAngel Princëzza LovërzNessuna valutazione finora
- Contrast EchocardiographyDocumento54 pagineContrast EchocardiographySruthiNessuna valutazione finora
- Measure Intracardiac Pressures & Assess Cardiac FunctionDocumento41 pagineMeasure Intracardiac Pressures & Assess Cardiac Functionwaleed315Nessuna valutazione finora
- Principles of Blood Transfusion 2Documento21 paginePrinciples of Blood Transfusion 2dhivya singhNessuna valutazione finora
- Simple Office SpirometryDocumento42 pagineSimple Office SpirometryRoberto Merza III100% (4)
- Physical ExaminationDocumento55 paginePhysical Examinationdakshpanchal26369Nessuna valutazione finora
- Blood Gas MachineDocumento33 pagineBlood Gas MachinenofearnofearNessuna valutazione finora
- Formula For Calculation of Hemodynamics in Cardiac Catheterization-Ver.1.1Documento3 pagineFormula For Calculation of Hemodynamics in Cardiac Catheterization-Ver.1.1Sam YenNessuna valutazione finora
- Pleural CollectionsDocumento30 paginePleural CollectionsRitam JoarderNessuna valutazione finora
- Vascular Acess Number 1Documento45 pagineVascular Acess Number 1Paulo GalangNessuna valutazione finora
- HBP C315HIS Implant Procedure-eLearnDocumento35 pagineHBP C315HIS Implant Procedure-eLearnRichiNessuna valutazione finora
- Intravenous fluid therapy monitoring for pharmacistsDocumento4 pagineIntravenous fluid therapy monitoring for pharmacistsjorge zuñigaNessuna valutazione finora
- Pulse Contour Cardiac Output Learning Package PDFDocumento17 paginePulse Contour Cardiac Output Learning Package PDFNurse PractitionerNessuna valutazione finora
- MonitoringDocumento128 pagineMonitoringShahzada irfanNessuna valutazione finora
- Ventilator Weaning and Spontaneous Breathing Trials An Educational Review 2016Documento7 pagineVentilator Weaning and Spontaneous Breathing Trials An Educational Review 2016Tarran PhagooNessuna valutazione finora
- Central Line PlacementDocumento49 pagineCentral Line PlacementAndresPimentelAlvarezNessuna valutazione finora
- Model SOP for Blood Component SeparationDocumento8 pagineModel SOP for Blood Component Separationayan CustodyNessuna valutazione finora
- Allen's TestDocumento2 pagineAllen's TestCee SanchezNessuna valutazione finora
- Vital Signs Guide - Measure Body Temp, BP, Pulse & MoreDocumento8 pagineVital Signs Guide - Measure Body Temp, BP, Pulse & MoreRicky LiNessuna valutazione finora
- Hemodynamic Parameters To Guide Fluid Therapy: Review Open AccessDocumento9 pagineHemodynamic Parameters To Guide Fluid Therapy: Review Open AccessIrma DamayantiNessuna valutazione finora
- Medical MirrorDocumento10 pagineMedical MirrorSHUBHAM GOVILNessuna valutazione finora
- Mechanical ThrombectomyDocumento58 pagineMechanical Thrombectomyres.uditacharyaNessuna valutazione finora
- Spirometry E-Guide 2013Documento28 pagineSpirometry E-Guide 2013Vidal Odon Ramos MermaNessuna valutazione finora
- Biomarkers For Myocardial Infarction, CVS BlockDocumento13 pagineBiomarkers For Myocardial Infarction, CVS BlockGlucose DRglucoseNessuna valutazione finora
- 2022 Pulse Oximetry and CapnographyDocumento33 pagine2022 Pulse Oximetry and CapnographyMohmmed MousaNessuna valutazione finora
- Facing Neu Ent Fearlessly: Ro AssessmDocumento7 pagineFacing Neu Ent Fearlessly: Ro AssessmokipashaNessuna valutazione finora
- Approach To The Patient in Shock: by James Holencik, DODocumento52 pagineApproach To The Patient in Shock: by James Holencik, DOLydia MamurNessuna valutazione finora
- Stroke Volume and Cardiac OutputDocumento2 pagineStroke Volume and Cardiac OutputDennifer MadayagNessuna valutazione finora
- Makalah HypertensionDocumento6 pagineMakalah HypertensionFatin ZafirahNessuna valutazione finora
- Intravenous Fluid Therapy in Critically Ill AdultsDocumento17 pagineIntravenous Fluid Therapy in Critically Ill AdultsntnquynhproNessuna valutazione finora
- A Guide To ECG Reporting For Year 3 Medical StudentsDocumento2 pagineA Guide To ECG Reporting For Year 3 Medical StudentscsngiuNessuna valutazione finora
- National ECG Workshop AIMST MMA 2015Documento217 pagineNational ECG Workshop AIMST MMA 2015Sara100% (1)
- Oxygen CascadeDocumento12 pagineOxygen Cascadehy3pjb1984Nessuna valutazione finora
- Normal Laboratory Values - Patient Test Reference RangesDocumento10 pagineNormal Laboratory Values - Patient Test Reference RangesGita Elisa Berlina GintingNessuna valutazione finora
- A Powerful Tool To Objectively Monitor Your Patients Ventilatory StatusDocumento36 pagineA Powerful Tool To Objectively Monitor Your Patients Ventilatory StatusBeth Strom-Sturm100% (1)
- MapseDocumento6 pagineMapseRaul GascueñaNessuna valutazione finora
- Viatom Product Catalog V1.4 20210702Documento22 pagineViatom Product Catalog V1.4 20210702minhnhat247Nessuna valutazione finora
- Cigna Medical Coverage Policy For Sleep Testing ServicesDocumento29 pagineCigna Medical Coverage Policy For Sleep Testing ServicesPhạm Văn HiệpNessuna valutazione finora
- Captopril Renography - Detect Renal Artery StenosisDocumento3 pagineCaptopril Renography - Detect Renal Artery StenosisSri HariNessuna valutazione finora
- E Posters PDFDocumento349 pagineE Posters PDFpriyadikkalaNessuna valutazione finora
- Cardiac CycleDocumento29 pagineCardiac CycleRussell Suter100% (1)
- Optiflow Presentation-Carly TorgersenDocumento12 pagineOptiflow Presentation-Carly Torgersenapi-252628311100% (1)
- Pre-op Evaluation SummaryDocumento1 paginaPre-op Evaluation Summarysabbo morsNessuna valutazione finora
- Intracranial Pressure: Dr. Akhmad Imron, Spbs Dept. of NeurosurgeryDocumento26 pagineIntracranial Pressure: Dr. Akhmad Imron, Spbs Dept. of Neurosurgeryandisti2323Nessuna valutazione finora
- Basics of Waveform Interpretation: RET 2284 Principles of Mechanical VentilationDocumento66 pagineBasics of Waveform Interpretation: RET 2284 Principles of Mechanical VentilationNanda MinndinNessuna valutazione finora
- ALP Testing SOPDocumento6 pagineALP Testing SOPUMMID WashimNessuna valutazione finora
- Doppler Ultrasound of The KidneysDocumento23 pagineDoppler Ultrasound of The KidneysivoklarinNessuna valutazione finora
- Mec-1200 VetDocumento2 pagineMec-1200 VetVinsmoke SanjiNessuna valutazione finora
- On Admission:: STROKE MANAGEMENT (Beaumont Hospital)Documento3 pagineOn Admission:: STROKE MANAGEMENT (Beaumont Hospital)Nadia SalwaniNessuna valutazione finora
- Design of Arterial Blood Pressure, Heart Rate Variability, and BRDocumento65 pagineDesign of Arterial Blood Pressure, Heart Rate Variability, and BRRafiul Huda RumelNessuna valutazione finora
- Celyon-293-LIT284 NIBP White Paper V5 - FinalDocumento9 pagineCelyon-293-LIT284 NIBP White Paper V5 - FinalBolawali KiNessuna valutazione finora
- Zy9100 TRM - SM - M1170718 - 002Documento159 pagineZy9100 TRM - SM - M1170718 - 002Manuel Flores0% (1)
- Harmony Vled PartsDocumento12 pagineHarmony Vled PartsManuel FloresNessuna valutazione finora
- Midmark Examination Table 222Documento170 pagineMidmark Examination Table 222Manuel FloresNessuna valutazione finora
- Hettich Rotofix 32 - User Manual PDFDocumento28 pagineHettich Rotofix 32 - User Manual PDFCarlosZapataNessuna valutazione finora
- Puritan Bennett 840 Service ManualDocumento540 paginePuritan Bennett 840 Service ManualNayke Vaz50% (2)
- Resectoscopio 8677 Richard WolfDocumento25 pagineResectoscopio 8677 Richard WolfManuel FloresNessuna valutazione finora
- User's Manual Ventilation SERVO-i/s Cleaning and MaintenanceDocumento38 pagineUser's Manual Ventilation SERVO-i/s Cleaning and MaintenancetallrajNessuna valutazione finora
- Technics SL 120 Owners ManualDocumento6 pagineTechnics SL 120 Owners ManualManuel FloresNessuna valutazione finora
- SERVOI SERVSPLIST Servo-I EN ALL PDFDocumento23 pagineSERVOI SERVSPLIST Servo-I EN ALL PDFManuel FloresNessuna valutazione finora
- Manual Edan 12Documento205 pagineManual Edan 12lineylosadagNessuna valutazione finora
- R Series Configuration Manual: 9650-0902-01 Rev. TDocumento96 pagineR Series Configuration Manual: 9650-0902-01 Rev. Tkevin alegreNessuna valutazione finora
- Manual System OneDocumento69 pagineManual System OneCarlos CortesNessuna valutazione finora
- Carl Zeiss FF 450 - en - 07.10.1996Documento50 pagineCarl Zeiss FF 450 - en - 07.10.1996Manuel FloresNessuna valutazione finora
- Cardiocare 2000 Operation ManualDocumento61 pagineCardiocare 2000 Operation ManualDokter MoezNessuna valutazione finora
- User-Manual-sunray SRF618B6Documento72 pagineUser-Manual-sunray SRF618B6Manuel FloresNessuna valutazione finora
- HP 8040A Fetal Monitor - User ManualDocumento28 pagineHP 8040A Fetal Monitor - User ManualManuel FloresNessuna valutazione finora
- Manuel4 acculan3TI PDFDocumento202 pagineManuel4 acculan3TI PDFManuel FloresNessuna valutazione finora
- R Series Configuration Manual: 9650-0902-01 Rev. TDocumento96 pagineR Series Configuration Manual: 9650-0902-01 Rev. Tkevin alegreNessuna valutazione finora
- Repair Instructions - Service No./Modi, Error ListDocumento153 pagineRepair Instructions - Service No./Modi, Error ListAbabil PragashNessuna valutazione finora
- Fiber Optic Laryngoscope Handles Directions For UseDocumento7 pagineFiber Optic Laryngoscope Handles Directions For UseManuel FloresNessuna valutazione finora
- Bionet BM3PatientMonitor - Service ManualDocumento61 pagineBionet BM3PatientMonitor - Service ManualIvan Berino0% (1)
- Drager-Narkomed - Service Manual PDFDocumento294 pagineDrager-Narkomed - Service Manual PDFCarolina SubiráNessuna valutazione finora
- Servo I OverviewDocumento23 pagineServo I OverviewManuel FloresNessuna valutazione finora
- Datex S5 - User ManualDocumento142 pagineDatex S5 - User ManualAndrea Nathaly Medina SanchezNessuna valutazione finora
- The Anesthesia Ventilator 8seitig en 101209 FinDocumento8 pagineThe Anesthesia Ventilator 8seitig en 101209 Finfalcone87Nessuna valutazione finora
- Mylab Seven CarateristicasDocumento12 pagineMylab Seven CarateristicasManuel Flores0% (1)
- Penlon Absorbedor A200Documento68 paginePenlon Absorbedor A200Manuel FloresNessuna valutazione finora
- Manual Tecnico MPC2050Documento1.171 pagineManual Tecnico MPC2050John Juquen100% (2)
- AO 820 Rotary Microtome User ManualDocumento8 pagineAO 820 Rotary Microtome User ManualAndres RestrepoNessuna valutazione finora
- LQ121S1DG31 TFT LCD ModuleDocumento19 pagineLQ121S1DG31 TFT LCD ModuleManuel FloresNessuna valutazione finora
- Syrgery Mock 2Documento8 pagineSyrgery Mock 2aa.Nessuna valutazione finora
- The Eckasha ActivationDocumento2 pagineThe Eckasha ActivationGavrila Lucian100% (1)
- Lecture 7. Developmental GeneticsDocumento25 pagineLecture 7. Developmental GeneticsJimmy BeastNessuna valutazione finora
- Medical Funnotes VolumeDocumento108 pagineMedical Funnotes VolumeChinNessuna valutazione finora
- 08 DN 005 BA Int OkDocumento64 pagine08 DN 005 BA Int OkvbogachevNessuna valutazione finora
- Neuromuscular Junction Blocking AgentsDocumento9 pagineNeuromuscular Junction Blocking AgentsSyvNessuna valutazione finora
- NURS1603 Course Outline PDFDocumento19 pagineNURS1603 Course Outline PDFYip Ka YiNessuna valutazione finora
- Secondary Growth of PlantsDocumento13 pagineSecondary Growth of PlantsAngie Kong Su Mei50% (2)
- Cysteine, Methionine, ProlineDocumento3 pagineCysteine, Methionine, ProlineRio BurlazaNessuna valutazione finora
- Excerpt From "Presence" by Amy CuddyDocumento10 pagineExcerpt From "Presence" by Amy CuddyOnPointRadioNessuna valutazione finora
- Rhopalocera (Butterfly) : FunctionsDocumento18 pagineRhopalocera (Butterfly) : FunctionsChris Anthony EdulanNessuna valutazione finora
- Pharmaceutics 09 00041 v2Documento14 paginePharmaceutics 09 00041 v2thasyaNessuna valutazione finora
- ABX Pentra 60-C Plus Analyzer - Service ManualDocumento314 pagineABX Pentra 60-C Plus Analyzer - Service ManualJose Rolando Orellana Rodriguez100% (2)
- 0 - 321113728 Chemistry Investigatory Project On Drugs Addiction Abuse PDFDocumento10 pagine0 - 321113728 Chemistry Investigatory Project On Drugs Addiction Abuse PDFPardhyuman Bhadu100% (1)
- Respiration in Plants: Key Terms and ProcessesDocumento12 pagineRespiration in Plants: Key Terms and ProcessesNalla Raghuram ChowdaryNessuna valutazione finora
- Porges-2003-The Polyvagal Theory-Phylogenetic Contributions To Social BehaviorDocumento11 paginePorges-2003-The Polyvagal Theory-Phylogenetic Contributions To Social BehaviorJohn Bakalis100% (1)
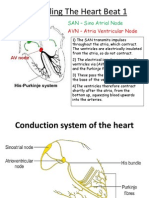
- Conduction System of HeartDocumento2 pagineConduction System of HeartEINSTEIN2DNessuna valutazione finora
- Chronic Cough Differential DiagnosisDocumento6 pagineChronic Cough Differential DiagnosisUbaidillah HafidzNessuna valutazione finora
- CK-MB production method reportDocumento1 paginaCK-MB production method reportOkura JoshuaNessuna valutazione finora
- General CharacteristicsDocumento24 pagineGeneral CharacteristicsdemanNessuna valutazione finora
- STD X - Biology - Paper VI FinalDocumento8 pagineSTD X - Biology - Paper VI FinalYashodhaNessuna valutazione finora
- Laryngeal ObstructionDocumento59 pagineLaryngeal ObstructionpravinNessuna valutazione finora
- Test 3 July 2018Documento8 pagineTest 3 July 2018Mobin Ur Rehman KhanNessuna valutazione finora
- Bacterial Culture Media: Classifying & Preparing Growth EnvironmentsDocumento8 pagineBacterial Culture Media: Classifying & Preparing Growth EnvironmentsawadsonNessuna valutazione finora
- Selection of Artificial TeethDocumento44 pagineSelection of Artificial TeethMohamed VandettaNessuna valutazione finora
- Human Motivation Edited2Documento23 pagineHuman Motivation Edited2jingoNessuna valutazione finora
- Benign Disorders of White Blood CellsDocumento31 pagineBenign Disorders of White Blood CellsjanNessuna valutazione finora
- Nci PBCF HTB22 - MCF7 - Sop 508 PDFDocumento26 pagineNci PBCF HTB22 - MCF7 - Sop 508 PDFmumu4loveNessuna valutazione finora
- UQU SLE CORRECTED FILE by DR Samina FidaDocumento537 pagineUQU SLE CORRECTED FILE by DR Samina Fidaasma .sassi100% (1)
- Unit 4 Knowledge Check 1Documento70 pagineUnit 4 Knowledge Check 1SH SNessuna valutazione finora