Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Achalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionDocumento10 pagineAchalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionJohnpeter EsporlasNessuna valutazione finora
- B. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactDocumento4 pagineB. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactJohnpeter EsporlasNessuna valutazione finora
- Bell's PalsyDocumento9 pagineBell's PalsyJohnpeter EsporlasNessuna valutazione finora
- Introduction To PharmacologyDocumento6 pagineIntroduction To PharmacologyJohnpeter EsporlasNessuna valutazione finora
- Amyotrophic Lateral SclerosisDocumento3 pagineAmyotrophic Lateral SclerosisJohnpeter EsporlasNessuna valutazione finora
- Pediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageDocumento3 paginePediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageJohnpeter EsporlasNessuna valutazione finora
- Is There Anything Left to Trust? - 40-character for document on trusting the BibleDocumento28 pagineIs There Anything Left to Trust? - 40-character for document on trusting the BibleJohnpeter EsporlasNessuna valutazione finora
- Assistive Devices RealDocumento3 pagineAssistive Devices RealJohnpeter EsporlasNessuna valutazione finora
- Mes 3Documento4 pagineMes 3Johnpeter EsporlasNessuna valutazione finora
- Parables of Jesus ChristDocumento4 pagineParables of Jesus ChristJohnpeter EsporlasNessuna valutazione finora
- Postpolio SyndromeDocumento3 paginePostpolio SyndromeJohnpeter Esporlas100% (1)
- ReviewDocumento10 pagineReviewJohnpeter EsporlasNessuna valutazione finora
- Tep 11 Reflexes PrintoutDocumento2 pagineTep 11 Reflexes PrintoutJohnpeter EsporlasNessuna valutazione finora
- Electrotherapy Parameters For Grand PraxDocumento3 pagineElectrotherapy Parameters For Grand PraxJohnpeter EsporlasNessuna valutazione finora
- Chapter 12Documento22 pagineChapter 12John EmmanuelNessuna valutazione finora
- KneeDocumento14 pagineKneeJohnpeter Esporlas100% (1)
- Patient Survey Results Guide Practice ImprovementsDocumento6 paginePatient Survey Results Guide Practice ImprovementsJohnpeter EsporlasNessuna valutazione finora
- TEP 2 Syllabus and Course Overviews for Physiotherapy ModulesDocumento2 pagineTEP 2 Syllabus and Course Overviews for Physiotherapy ModulesJohnpeter EsporlasNessuna valutazione finora
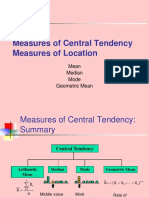
- Central TendencyDocumento25 pagineCentral TendencyJohnpeter EsporlasNessuna valutazione finora
- SHOULDER PAIN AND INJURY GUIDEDocumento7 pagineSHOULDER PAIN AND INJURY GUIDEJohnpeter EsporlasNessuna valutazione finora
- Neuroanatomy Pictures Part 2 - WaxmanDocumento6 pagineNeuroanatomy Pictures Part 2 - WaxmanJohnpeter EsporlasNessuna valutazione finora
- CVA - Compilation of All BooksDocumento4 pagineCVA - Compilation of All BooksJohnpeter EsporlasNessuna valutazione finora
- Down SyndromeDocumento2 pagineDown SyndromeJohnpeter EsporlasNessuna valutazione finora
- CBR Topic Outline 2017-2018Documento3 pagineCBR Topic Outline 2017-2018Johnpeter EsporlasNessuna valutazione finora
- Cardiovascular RehabilitationDocumento5 pagineCardiovascular RehabilitationJohnpeter EsporlasNessuna valutazione finora
- Etiology, Epidemiology & Differential Diagnosis For CADDocumento9 pagineEtiology, Epidemiology & Differential Diagnosis For CADJohnpeter EsporlasNessuna valutazione finora
- Atlas of Digestive SystemDocumento3 pagineAtlas of Digestive SystemJohnpeter EsporlasNessuna valutazione finora
- Normal Body TemperaturesDocumento5 pagineNormal Body TemperaturesJohnpeter EsporlasNessuna valutazione finora
- Anthropometric SDocumento3 pagineAnthropometric SJohnpeter EsporlasNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Fructus SchisandraeDocumento14 pagineFructus SchisandraeHenrique Santa Capita CerqueiraNessuna valutazione finora
- Cellular Adaptation-1Documento8 pagineCellular Adaptation-1abdo100% (1)
- Tachdjian's Pediatric Orthopaedics v.4Documento660 pagineTachdjian's Pediatric Orthopaedics v.4Leonardo Garay QuinteroNessuna valutazione finora
- Pathology-1 (Introduction To Pathology)Documento87 paginePathology-1 (Introduction To Pathology)Durge Raj Ghalan67% (6)
- Introduction and Neoplasia - PathologyDocumento20 pagineIntroduction and Neoplasia - PathologyjmosserNessuna valutazione finora
- Cellular Adaptations & Growth DisturbancesDocumento27 pagineCellular Adaptations & Growth DisturbancesJames MubitahNessuna valutazione finora
- Cell Injury, Cell Death, and Adaptations 13-2-15Documento34 pagineCell Injury, Cell Death, and Adaptations 13-2-15DrSyeda Rima100% (2)
- The Exerkine Apelin Reverses Age-Associated Sarcopenia: ArticlesDocumento18 pagineThe Exerkine Apelin Reverses Age-Associated Sarcopenia: ArticlesJuniorMartinsNessuna valutazione finora
- Cellular Adaptation & Pathologic ChangesDocumento2 pagineCellular Adaptation & Pathologic ChangesChe Ainun Nasihah IsmailNessuna valutazione finora
- Medical Terminology For Health Care Professionals A Word Building Approach 9Th Edition Rice Test Bank Full Chapter PDFDocumento62 pagineMedical Terminology For Health Care Professionals A Word Building Approach 9Th Edition Rice Test Bank Full Chapter PDFDebraBurtonkfmanNessuna valutazione finora
- Rehab Medik - Dr. Joudy Gessal, SPRM - Modul Penurunan KesadaranDocumento17 pagineRehab Medik - Dr. Joudy Gessal, SPRM - Modul Penurunan KesadaranRian Candra IbrahimNessuna valutazione finora
- Nasa Pemf Slisci 12Documento2 pagineNasa Pemf Slisci 12Homers SimpsonNessuna valutazione finora
- Lesson 4: Fixation and FixativesDocumento23 pagineLesson 4: Fixation and FixativesMary GNessuna valutazione finora
- Wei SyndromeDocumento8 pagineWei SyndromeezraallenNessuna valutazione finora
- Pathology of Peripheral Nerve and Skeletal Muscle - DADocumento46 paginePathology of Peripheral Nerve and Skeletal Muscle - DASinta Dewi AdityaniNessuna valutazione finora
- Year 2 NotesDocumento1.495 pagineYear 2 Notesjmosser100% (3)
- Zalavadiya Jinal GirishbhaiDocumento4 pagineZalavadiya Jinal GirishbhaiJinalNessuna valutazione finora
- Muscle BiopsyDocumento162 pagineMuscle BiopsyYerko IvánovicNessuna valutazione finora
- Atrophy, Testis Normal HistologyDocumento4 pagineAtrophy, Testis Normal Histologytaisharose lisondraNessuna valutazione finora
- Student Notes: GPHCT: Davao Doctors College Medical Laboratory Science DepartmentDocumento30 pagineStudent Notes: GPHCT: Davao Doctors College Medical Laboratory Science DepartmentMimi EcleoNessuna valutazione finora
- 500 SBA Gen SystemicDocumento27 pagine500 SBA Gen Systemicdr_shafiqNessuna valutazione finora
- Robbins Pathology - Chapter 2 TransDocumento19 pagineRobbins Pathology - Chapter 2 Transnath nath100% (3)
- Cellular responses to stress and toxic insultsDocumento29 pagineCellular responses to stress and toxic insultsMK100% (1)
- Atrophic RhinitisDocumento11 pagineAtrophic Rhinitiskiruthiga.sNessuna valutazione finora
- Cellular Adaptations to StressDocumento4 pagineCellular Adaptations to StressShealtiel MajadasNessuna valutazione finora
- Cellular AdaptationsDocumento66 pagineCellular AdaptationsShivan UmamaheswaranNessuna valutazione finora
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocumento20 pagineHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNessuna valutazione finora
- Morphea-Like Lesions After Botulinum Toxin A Injections: Ase SeriesDocumento3 pagineMorphea-Like Lesions After Botulinum Toxin A Injections: Ase Seriesirwan junNessuna valutazione finora
- 3 Muscle Pathology in Free-Ranging StrandedDocumento14 pagine3 Muscle Pathology in Free-Ranging StrandedXimena RomeroNessuna valutazione finora
- Skeletal Muscle Atrophy & Immobility EffectsDocumento42 pagineSkeletal Muscle Atrophy & Immobility EffectsErrolNessuna valutazione finora