Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- EMP Enero 2011 Anticoagulacioìn en UrgenciaDocumento20 pagineEMP Enero 2011 Anticoagulacioìn en UrgenciaNicolás HerreraNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Study Guide NREMTDocumento4 pagineStudy Guide NREMTdebbiemedic355725% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Lord of The FliesDocumento9 pagineLord of The FliesKarson TangNessuna valutazione finora
- NHS Highland Wound Management Guidelines and Formulary PDFDocumento91 pagineNHS Highland Wound Management Guidelines and Formulary PDFubayyumr100% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Bones PDFDocumento227 pagineBones PDFAtthapu ThirupathaiahNessuna valutazione finora
- Gingival RecessionDocumento22 pagineGingival RecessionAsmita Wankhede MeshramNessuna valutazione finora
- Rosenberg AcupointsDocumento4 pagineRosenberg AcupointsxnrvNessuna valutazione finora
- TOEFL Vocabulary Quiz Book PDFDocumento364 pagineTOEFL Vocabulary Quiz Book PDFAngga Saputra100% (1)
- Lilius vs. Manila Railroad Co., 62 Phil. 56Documento4 pagineLilius vs. Manila Railroad Co., 62 Phil. 56Francise Mae Montilla MordenoNessuna valutazione finora
- Lipke Second EditionDocumento194 pagineLipke Second EditionDavid Wrobel100% (7)
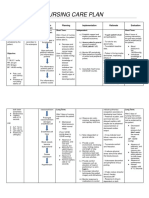
- Nursing Care Plan For HELLP SyndromeDocumento17 pagineNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Radicular CystDocumento1 paginaRadicular CystNadya Pratiwi UtamiNessuna valutazione finora
- KompositDocumento6 pagineKompositHanny HoneyyNessuna valutazione finora
- Maturo GenesisDocumento7 pagineMaturo GenesisHanny HoneyyNessuna valutazione finora
- Jurnal-6-Naskah 2 JURNAL PDGI Vol 61 No 1Documento5 pagineJurnal-6-Naskah 2 JURNAL PDGI Vol 61 No 1Hanny HoneyyNessuna valutazione finora
- EfewDocumento1 paginaEfewHanny HoneyyNessuna valutazione finora
- Jurnal-3-Naskah 6 JURNAL PDGI Vol 59 No 1Documento6 pagineJurnal-3-Naskah 6 JURNAL PDGI Vol 59 No 1thiewyNessuna valutazione finora
- Dental Research JournalDocumento28 pagineDental Research JournalHanny HoneyyNessuna valutazione finora
- YeDocumento1 paginaYeHanny HoneyyNessuna valutazione finora
- Effect of Staining Agents On Color Change of CompositesDocumento6 pagineEffect of Staining Agents On Color Change of CompositesHanny HoneyyNessuna valutazione finora
- ReferenceDocumento2 pagineReferenceHanny HoneyyNessuna valutazione finora
- EfewDocumento1 paginaEfewHanny HoneyyNessuna valutazione finora
- Praktikum 10Documento2 paginePraktikum 10Hanny HoneyyNessuna valutazione finora
- Beberapa Indeks Maloklusi: Author: Thalca AgusniDocumento1 paginaBeberapa Indeks Maloklusi: Author: Thalca Agusniavinandri mantrasariNessuna valutazione finora
- Beberapa Indeks Maloklusi: Author: Thalca AgusniDocumento1 paginaBeberapa Indeks Maloklusi: Author: Thalca Agusniavinandri mantrasariNessuna valutazione finora
- Praktikum 1Documento2 paginePraktikum 1Hanny HoneyyNessuna valutazione finora
- Nonparametric Correlations: NotesDocumento2 pagineNonparametric Correlations: NotesHanny HoneyyNessuna valutazione finora
- Praktikum 5Documento7 paginePraktikum 5Hanny HoneyyNessuna valutazione finora
- Npar Tests: New File. Dataset Name Dataset5 Window Front. Npar Tests /M-W Skor by JK (1 2) /missing AnalysisDocumento2 pagineNpar Tests: New File. Dataset Name Dataset5 Window Front. Npar Tests /M-W Skor by JK (1 2) /missing AnalysisHanny HoneyyNessuna valutazione finora
- Npar Tests: New File. Dataset Name Dataset6 Window Front. Npar Tests /K-W Skor by Kel (1 3) /missing AnalysisDocumento2 pagineNpar Tests: New File. Dataset Name Dataset6 Window Front. Npar Tests /K-W Skor by Kel (1 3) /missing AnalysisHanny HoneyyNessuna valutazione finora
- Praktikum 2Documento4 paginePraktikum 2Hanny HoneyyNessuna valutazione finora
- Body Composition: Prof Dwi PrijatmokoDocumento35 pagineBody Composition: Prof Dwi PrijatmokoHanny HoneyyNessuna valutazione finora
- Praktikum 4Documento2 paginePraktikum 4Hanny HoneyyNessuna valutazione finora
- Praktikum 3Documento2 paginePraktikum 3Hanny HoneyyNessuna valutazione finora
- Mammal Skeleton Functions & RegionsDocumento19 pagineMammal Skeleton Functions & RegionsPenelope May MorkelNessuna valutazione finora
- Biology Reflexes and Reactions LabDocumento2 pagineBiology Reflexes and Reactions LabKiran Raj RNessuna valutazione finora
- Flixborough DisasterDocumento4 pagineFlixborough DisasterEddylyn MarieNessuna valutazione finora
- Drowning CaseDocumento3 pagineDrowning CaseMiranda NasutionNessuna valutazione finora
- 96-8000L English Mill Operator PDFDocumento207 pagine96-8000L English Mill Operator PDFThomson SimanjuntakNessuna valutazione finora
- Low Back Pain Dr. Hardhi PRanataDocumento57 pagineLow Back Pain Dr. Hardhi PRanataPerwita ArumingtyasNessuna valutazione finora
- Harry Potter SpellsDocumento21 pagineHarry Potter SpellsSotiris Pappas100% (1)
- Heat Generated by Dental Implant Drills During Osteotomy - A Review-SKumarMishraDocumento13 pagineHeat Generated by Dental Implant Drills During Osteotomy - A Review-SKumarMishraanilsamuel0077418Nessuna valutazione finora
- Distal Radius Fractures With Ulnar Styloid Fracture - V2Documento30 pagineDistal Radius Fractures With Ulnar Styloid Fracture - V2Chinmaye PurushothamNessuna valutazione finora
- Endodontic Surgery: Incision and DrainageDocumento8 pagineEndodontic Surgery: Incision and DrainageHadoo OolaNessuna valutazione finora
- Nursing Care PlansDocumento6 pagineNursing Care PlansjessamariesabioNessuna valutazione finora
- Osteoarthritis Genu RehabilitationDocumento52 pagineOsteoarthritis Genu Rehabilitationwahyu_sitaNessuna valutazione finora
- Yamaha Gp1200 Owners ManualDocumento3 pagineYamaha Gp1200 Owners ManualGregoryNessuna valutazione finora
- Dutchess County: Traffic Safety DataDocumento30 pagineDutchess County: Traffic Safety DataDaily FreemanNessuna valutazione finora
- Obstetric Anatomy: Professor of Obstetrics & Gynecology Ain Shams Faculty of MedicineDocumento67 pagineObstetric Anatomy: Professor of Obstetrics & Gynecology Ain Shams Faculty of MedicineJoan LuisNessuna valutazione finora
- 12" Bench Drill Press: (Model DP300)Documento17 pagine12" Bench Drill Press: (Model DP300)xlotoxNessuna valutazione finora
- Chest Drains GuidanceDocumento14 pagineChest Drains Guidancenob2011nobNessuna valutazione finora
- Risk Assesment For StudioDocumento5 pagineRisk Assesment For StudioaishahkhanNessuna valutazione finora
- Stanley MBX138-MBX608 English User Manual 2-2016Documento62 pagineStanley MBX138-MBX608 English User Manual 2-2016luismdmj100% (1)
- SC-2103681-ME1a - Manual 660.YTC. (1x6.5kW) .6 M1546-51G K460-4522-12FO-FC-R M9PG-OT-WP-LCBT + DG90-DB120 + 2xDG45 4xM1Documento61 pagineSC-2103681-ME1a - Manual 660.YTC. (1x6.5kW) .6 M1546-51G K460-4522-12FO-FC-R M9PG-OT-WP-LCBT + DG90-DB120 + 2xDG45 4xM1kiên phạm trungNessuna valutazione finora
- Neb-Pmdc Step 2 Past Papers by Dr. Asif Ali PDFDocumento54 pagineNeb-Pmdc Step 2 Past Papers by Dr. Asif Ali PDFZaraNessuna valutazione finora