Potrebbero piacerti anche
- Colloidal Silver Cures MRSA ReportDocumento16 pagineColloidal Silver Cures MRSA ReportGodwinNessuna valutazione finora
- Lipids Case StudiesDocumento6 pagineLipids Case Studiesgogo29% (7)
- Fundamentals and Applications of Controlled Release Drug Delivery PDFDocumento607 pagineFundamentals and Applications of Controlled Release Drug Delivery PDFTurco Sekoof50% (2)
- Nicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFDocumento927 pagineNicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFJamie Baczewski100% (8)
- Fast Facts: Hyperlipidemia: Bringing clarity to lipid managementDa EverandFast Facts: Hyperlipidemia: Bringing clarity to lipid managementNessuna valutazione finora
- Normal ValuesDocumento1 paginaNormal ValuesmimNessuna valutazione finora
- Awareness Under AnesthesiaDocumento27 pagineAwareness Under AnesthesiaagatakassaNessuna valutazione finora
- L46 - Whitefield Lab Home Visit Sy No. 18/1B, K R Puram, Hobli, Sree Sai Harsha Tower, White FieldDocumento4 pagineL46 - Whitefield Lab Home Visit Sy No. 18/1B, K R Puram, Hobli, Sree Sai Harsha Tower, White FieldSayantan BanerjeeNessuna valutazione finora
- Independent Nurse PractitionerDocumento4 pagineIndependent Nurse PractitionerVijith.V.kumar50% (2)
- Sepsis, Septic Shock, MODSDocumento19 pagineSepsis, Septic Shock, MODSPaul Zantua80% (5)
- Anesthesiology MnemonicsDocumento1 paginaAnesthesiology MnemonicsMartin Susanto, MD100% (3)
- MG/DL MG/DL MG/DL MG/DL MG/DL MG/DLDocumento3 pagineMG/DL MG/DL MG/DL MG/DL MG/DL MG/DLAli Shaikh AbdulNessuna valutazione finora
- MG/DL MG/DL MG/DL MG/DL MG/DLDocumento2 pagineMG/DL MG/DL MG/DL MG/DL MG/DLsureshNessuna valutazione finora
- DRRKDocumento1 paginaDRRKrevanth kallaNessuna valutazione finora
- Reference Group Reference Range in NG/MLDocumento2 pagineReference Group Reference Range in NG/MLAbhishek AroraNessuna valutazione finora
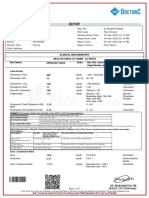
- Lipid Profile: Test Name Result Units Biological Reference IntervalDocumento2 pagineLipid Profile: Test Name Result Units Biological Reference IntervalArpanpatelNessuna valutazione finora
- Sameera-18Sep2022-Health CheDocumento5 pagineSameera-18Sep2022-Health CheElias JhakiNessuna valutazione finora
- Lipids & Lipoproteins: Cc-Lecture by Dianne Jagonia, RMTDocumento32 pagineLipids & Lipoproteins: Cc-Lecture by Dianne Jagonia, RMTMarl EstradaNessuna valutazione finora
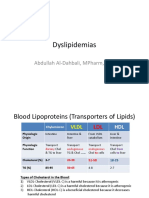
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocumento15 pagineDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNessuna valutazione finora
- Drugs Affecting Lipid MetabolismDocumento50 pagineDrugs Affecting Lipid MetabolismchiragcvpNessuna valutazione finora
- FC0850661Documento1 paginaFC0850661SK FahimNessuna valutazione finora
- Sample Type: Serum Client Address:: Obtained ValueDocumento1 paginaSample Type: Serum Client Address:: Obtained Valuesrini vasuNessuna valutazione finora
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Documento20 pagineTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNessuna valutazione finora
- CC Reference ValuesDocumento2 pagineCC Reference ValuesJoan ClaveNessuna valutazione finora
- Report (5) DasuDocumento1 paginaReport (5) DasuDasu GundiNessuna valutazione finora
- LipidDocumento1 paginaLipidrajanarora72Nessuna valutazione finora
- Estimation of Serum CholesterolDocumento44 pagineEstimation of Serum CholesterolHasan ShahriarNessuna valutazione finora
- Alfa ResultSubServices 4Documento1 paginaAlfa ResultSubServices 4ayaabouaufNessuna valutazione finora
- Test Name Result Unit Bio Ref. Interval Method: Glucose, FastingDocumento6 pagineTest Name Result Unit Bio Ref. Interval Method: Glucose, FastingDeepneel KunduNessuna valutazione finora
- Pto LamaDocumento5 paginePto LamaAyu MawariNessuna valutazione finora
- Gias Uddin Ansary 2Documento2 pagineGias Uddin Ansary 2Rezaul KarimNessuna valutazione finora
- Brahmeshwar Ojha 425733 13-02-2023 20230213060533 StationerypdfmergedDocumento11 pagineBrahmeshwar Ojha 425733 13-02-2023 20230213060533 StationerypdfmergedAmaresh ojhaNessuna valutazione finora
- LgedhrrhfDocumento24 pagineLgedhrrhfkgavila1955pamNessuna valutazione finora
- Lipid Biokimia Semester 2Documento93 pagineLipid Biokimia Semester 2Anonymous oyAUZoCeyNessuna valutazione finora
- Ann Soehee - Tctap2021 - SPCDocumento43 pagineAnn Soehee - Tctap2021 - SPCSaad KhanNessuna valutazione finora
- MNT-Dislipidemia-Unja 20022019 PDFDocumento48 pagineMNT-Dislipidemia-Unja 20022019 PDFAnonymous o3Q3QXENessuna valutazione finora
- SVLT Lab Report DetailsDocumento3 pagineSVLT Lab Report Detailspancard1098Nessuna valutazione finora
- Newscan 2023 09 25 - 083731Documento2 pagineNewscan 2023 09 25 - 083731Hilal HazaaNessuna valutazione finora
- Clinical Chemistry Report 07-03-2022Documento1 paginaClinical Chemistry Report 07-03-2022RB STNessuna valutazione finora
- Lab ReportDocumento2 pagineLab ReportGopinath K.PNessuna valutazione finora
- Cholesterol Risk TableDocumento2 pagineCholesterol Risk TableFahad Shah JehanNessuna valutazione finora
- Alfa ResultSubServicesDocumento1 paginaAlfa ResultSubServicesbqmp886xyqNessuna valutazione finora
- Lipid ProfileDocumento20 pagineLipid Profileمحمد هزاع الصبريNessuna valutazione finora
- Complete Blood Count Red Blood Cell (RBC) : M: 4.5 - 5.5 F: 4.0 - 4.9 x10 /MLDocumento6 pagineComplete Blood Count Red Blood Cell (RBC) : M: 4.5 - 5.5 F: 4.0 - 4.9 x10 /MLMel-Hanie MabatasNessuna valutazione finora
- Chemistry Unit: Cholest./HDL/LDL/TriglyceridesDocumento1 paginaChemistry Unit: Cholest./HDL/LDL/TriglyceridesMAHMOUDNessuna valutazione finora
- Biochemistry "Lipids Test"Documento8 pagineBiochemistry "Lipids Test"HERONessuna valutazione finora
- LabReport L1 MR - SEELAMESOBU45YRS M 02 06 202320230602 2 s259rfDocumento1 paginaLabReport L1 MR - SEELAMESOBU45YRS M 02 06 202320230602 2 s259rfNanda Gopal Reddy AnamNessuna valutazione finora
- Alfa ResultSubServicesDocumento1 paginaAlfa ResultSubServicesOsman OsmanNessuna valutazione finora
- NCEP Hyperlipidemia GoalsDocumento6 pagineNCEP Hyperlipidemia GoalsVictoria Eliza InguilloNessuna valutazione finora
- Lodo TopnoDocumento4 pagineLodo TopnoGautam DxNessuna valutazione finora
- Bio ,, OSPEDocumento10 pagineBio ,, OSPEOsama BakheetNessuna valutazione finora
- Familial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Documento43 pagineFamilial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Gourav Kumar SinhaNessuna valutazione finora
- Biochemistry: Laboratory ReportDocumento4 pagineBiochemistry: Laboratory ReportChithraa KarthikNessuna valutazione finora
- Pt's Name Ref - By:: Vinayswami C/o. Self.: Lipid ProfileDocumento1 paginaPt's Name Ref - By:: Vinayswami C/o. Self.: Lipid ProfileArpanpatelNessuna valutazione finora
- HyperlipidemiaDocumento33 pagineHyperlipidemiaHimaNessuna valutazione finora
- 4.investigations of Serum LipidsDocumento7 pagine4.investigations of Serum LipidsMV ProductionNessuna valutazione finora
- Lipid Profile L - DeterminatinDocumento33 pagineLipid Profile L - DeterminatinaliNessuna valutazione finora
- Anti-Hyperlipidemic Agents: Topics of Special InterestDocumento10 pagineAnti-Hyperlipidemic Agents: Topics of Special InterestMuhammad Kamran BalochNessuna valutazione finora
- Glycosylated HB (Hba1C) 7.2 Mean Plasma Glucose Level During The Last 3 Months 160Documento2 pagineGlycosylated HB (Hba1C) 7.2 Mean Plasma Glucose Level During The Last 3 Months 160ammar88egyNessuna valutazione finora
- Parvez Jamal 68935922024 01 20 02 04 33 422 6 0 1 114 133502373061826411 PDFDocumento3 pagineParvez Jamal 68935922024 01 20 02 04 33 422 6 0 1 114 133502373061826411 PDFMaref JamalNessuna valutazione finora
- Rafeek T - 134569Documento1 paginaRafeek T - 134569rafeeqabdulla50772785Nessuna valutazione finora
- IRON - Ferrozine Total Iron Binding Capacity (Tibc) - Calculated % Transferrin Saturation - CalculatedDocumento13 pagineIRON - Ferrozine Total Iron Binding Capacity (Tibc) - Calculated % Transferrin Saturation - CalculatedEmami RosscareNessuna valutazione finora
- Lipids and Lipoproteins in Blood Plasma (Serum) : Mayo Clinic Laboratories Cardiovascular Laboratory MedicineDocumento4 pagineLipids and Lipoproteins in Blood Plasma (Serum) : Mayo Clinic Laboratories Cardiovascular Laboratory MedicineMudassar SattarNessuna valutazione finora
- Main Lab, ISB: Sumbaleen Mudassir HD-17725Documento1 paginaMain Lab, ISB: Sumbaleen Mudassir HD-17725Mudassir IqbalNessuna valutazione finora
- IRON - Ferrozine Total Iron Binding Capacity (Tibc) - Calculated % Transferrin Saturation - CalculatedDocumento13 pagineIRON - Ferrozine Total Iron Binding Capacity (Tibc) - Calculated % Transferrin Saturation - CalculatedEmami RosscareNessuna valutazione finora
- 52 Year Male 72622503798: Patient NameDocumento1 pagina52 Year Male 72622503798: Patient NameMahmoud HosniNessuna valutazione finora
- BCMTMS Practice Exam Answers PDF 2023Documento61 pagineBCMTMS Practice Exam Answers PDF 2023TammyNessuna valutazione finora
- Laboratory Procedure ManualDocumento23 pagineLaboratory Procedure ManualIseth ISethNessuna valutazione finora
- SRSP30Documento23 pagineSRSP30Priyanshu UpadhyayNessuna valutazione finora
- পা পিছলে ইঞ্জিনিয়ারDocumento10 pagineপা পিছলে ইঞ্জিনিয়ারSayantan BanerjeeNessuna valutazione finora
- ESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Documento14 pagineESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Sayantan BanerjeeNessuna valutazione finora
- Govt Exam Previous Year Model Question Papers With Answer Key PDF 08Documento29 pagineGovt Exam Previous Year Model Question Papers With Answer Key PDF 08Sayantan Banerjee100% (1)
- Apdf A 1094175 e 1 U 1186466Documento2 pagineApdf A 1094175 e 1 U 1186466Sayantan BanerjeeNessuna valutazione finora
- Raju DasDocumento1 paginaRaju DasSayantan BanerjeeNessuna valutazione finora
- Instructions For The Shortlisted Candidates 11072017Documento2 pagineInstructions For The Shortlisted Candidates 11072017Sayantan BanerjeeNessuna valutazione finora
- ESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Documento14 pagineESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Sayantan BanerjeeNessuna valutazione finora
- CGL Tier 1 2014 Exam PaperDocumento21 pagineCGL Tier 1 2014 Exam PaperGaurav KumarNessuna valutazione finora
- NIELIT Recruitment For Scientist and Technical Assistants 2017 Official NotificationDocumento6 pagineNIELIT Recruitment For Scientist and Technical Assistants 2017 Official NotificationKshitija100% (1)
- ITProjection 2017-2018 BDocumento2 pagineITProjection 2017-2018 BSayantan BanerjeeNessuna valutazione finora
- ITProjection 2017-2018Documento2 pagineITProjection 2017-2018Sayantan BanerjeeNessuna valutazione finora
- Bal Bal BalDocumento1 paginaBal Bal BalSayantan BanerjeeNessuna valutazione finora
- ESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Documento14 pagineESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Sayantan BanerjeeNessuna valutazione finora
- ESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Documento14 pagineESSAY TOPIC: Jan Dhan Yojana: Fifty Gold in Olympics: Can This Be A Reality For India?Sayantan BanerjeeNessuna valutazione finora
- Solved PrecisDocumento6 pagineSolved PrecisYehyaKhanNessuna valutazione finora
- Admit Card VSPDocumento2 pagineAdmit Card VSPSayantan BanerjeeNessuna valutazione finora
- Transco Electrical and Electronics Engineering SET ADocumento16 pagineTransco Electrical and Electronics Engineering SET Aishak789Nessuna valutazione finora
- Coal India Exam Leave Rules 2010 PDFDocumento23 pagineCoal India Exam Leave Rules 2010 PDFSayantan BanerjeeNessuna valutazione finora
- Electrical Engineering QuestionDocumento11 pagineElectrical Engineering QuestionDavid RahulNessuna valutazione finora
- APTRANCOSub-Engineer Electrical UnlockedDocumento16 pagineAPTRANCOSub-Engineer Electrical UnlockedSayantan BanerjeeNessuna valutazione finora
- Coal India Exam Leave Rules 2010 PDFDocumento23 pagineCoal India Exam Leave Rules 2010 PDFSayantan BanerjeeNessuna valutazione finora
- 23 Techniques PDFDocumento25 pagine23 Techniques PDFsdhineshbe100% (1)
- SSC Capsule 2016 PDFDocumento97 pagineSSC Capsule 2016 PDFAnuj PrakashNessuna valutazione finora
- BSNL JE Earstwhile TTA Result 2016Documento45 pagineBSNL JE Earstwhile TTA Result 2016Amol Kore-MaliNessuna valutazione finora
- Quality Form BDocumento10 pagineQuality Form BFranz ToledoNessuna valutazione finora
- Reten Modern Dressing 2023 PKDMTDocumento51 pagineReten Modern Dressing 2023 PKDMTMasros TukiranNessuna valutazione finora
- Ancient Greece and Ancient Rome InfographicDocumento1 paginaAncient Greece and Ancient Rome InfographicearliscutelikeomgNessuna valutazione finora
- Kci Vac Therapy Vtiaf UpdatedDocumento2 pagineKci Vac Therapy Vtiaf UpdatedHi BeyoNessuna valutazione finora
- Sample Leave Restriction LetterDocumento3 pagineSample Leave Restriction LetterGayathriNessuna valutazione finora
- Drugs Dosage Nursing Implications: Discharge PlanDocumento2 pagineDrugs Dosage Nursing Implications: Discharge PlanCristina L. JaysonNessuna valutazione finora
- Pcod 0343021025 PDFDocumento5 paginePcod 0343021025 PDFArun AchalamNessuna valutazione finora
- Basics Concept of Pharmacoepidemiology: Yusi AnggrianiDocumento21 pagineBasics Concept of Pharmacoepidemiology: Yusi AnggrianiDjuffiNelwanNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaIntania MairudiNessuna valutazione finora
- The Law Is Changing FAQs On ScriptCheckSADocumento4 pagineThe Law Is Changing FAQs On ScriptCheckSAYusri KardoNessuna valutazione finora
- COVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online SurveyDocumento10 pagineCOVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online Surveyh3493061Nessuna valutazione finora
- Flabby Alveolar Ridges: A Modified Technique To Treat This Clinical ChallengeDocumento4 pagineFlabby Alveolar Ridges: A Modified Technique To Treat This Clinical ChallengeammarkochiNessuna valutazione finora
- Arsenic - IARC Monograph V84Documento526 pagineArsenic - IARC Monograph V84ACNessuna valutazione finora
- Weekend - Holiday Physiotherapy Prioritization GuidelinesDocumento1 paginaWeekend - Holiday Physiotherapy Prioritization GuidelinesDavid ComeauNessuna valutazione finora
- Smart Multi Critical Care Brochure PDFDocumento17 pagineSmart Multi Critical Care Brochure PDFNickLooNessuna valutazione finora
- Treatment Center PDFDocumento120 pagineTreatment Center PDFShellyNessuna valutazione finora
- Fitness & Wellness Industry in IndiaDocumento12 pagineFitness & Wellness Industry in IndiaPrince SinghNessuna valutazione finora
- Ncp-Case Pre Impaired Tissue Integrity-1Documento2 pagineNcp-Case Pre Impaired Tissue Integrity-1Jade HemmingsNessuna valutazione finora
- Surveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDocumento28 pagineSurveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDebNessuna valutazione finora
- Applications of Biotechnology in HealthDocumento21 pagineApplications of Biotechnology in Healtherinliannamanalad4210Nessuna valutazione finora
- Unit 10Documento22 pagineUnit 10hafizur rahmanNessuna valutazione finora
- VVND TreatmentDocumento4 pagineVVND Treatmentkarthivisu2009100% (1)
- Ulkus VarricosumDocumento26 pagineUlkus VarricosumNurul FadilahNessuna valutazione finora