Potrebbero piacerti anche
- Sce Gastro Sample QsDocumento36 pagineSce Gastro Sample QsZoya Annam100% (8)
- An Introduction To Autopsy Technique: Step-by-Step DiagramsDocumento24 pagineAn Introduction To Autopsy Technique: Step-by-Step Diagramskarin45Nessuna valutazione finora
- Chronic Liver DiseaseDocumento30 pagineChronic Liver Diseaseprajwal86% (7)
- Vascular Diseases (1 of 3)Documento4 pagineVascular Diseases (1 of 3)Doctor GeneralNessuna valutazione finora
- Hepatic Surgical AnatomyDocumento23 pagineHepatic Surgical Anatomyyacine26Nessuna valutazione finora
- Extrahepatic CholestasisDocumento31 pagineExtrahepatic CholestasismackieccNessuna valutazione finora
- Acute Scrotum Guide: Diagnosing and Treating Urological EmergenciesDocumento25 pagineAcute Scrotum Guide: Diagnosing and Treating Urological EmergenciesFidelis Lovely100% (1)
- To TiroidDocumento67 pagineTo TiroidfaisaldanyaniNessuna valutazione finora
- Gastrointestinal Anatomy and Physiology: The EssentialsDa EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNessuna valutazione finora
- Mirizzi Syndrome - UpToDateDocumento15 pagineMirizzi Syndrome - UpToDateEdgar Miguel ContrerasNessuna valutazione finora
- Gallstone Disease and Acute Cholecystitis MADDocumento21 pagineGallstone Disease and Acute Cholecystitis MADMuhammad AbdurrahmanNessuna valutazione finora
- Liver Cirrhosis LectureDocumento83 pagineLiver Cirrhosis LectureSheila Regina Tiza100% (1)
- GI NotesDocumento19 pagineGI NotesBigBoostingNessuna valutazione finora
- OS205 Cardiac ImagingDocumento7 pagineOS205 Cardiac ImagingLaurisse ManaloNessuna valutazione finora
- Quizlet EndoDocumento17 pagineQuizlet EndoemmaNessuna valutazione finora
- Congenital Anomalies of Urinary BladderDocumento102 pagineCongenital Anomalies of Urinary Bladdernancy voraNessuna valutazione finora
- Bladder Outlet Obstruction in Children PDFDocumento64 pagineBladder Outlet Obstruction in Children PDFalaaNessuna valutazione finora
- Billiary SystemDocumento60 pagineBilliary SystemDONALD UNASHENessuna valutazione finora
- Surgical Specialties DR - PaghubasanDocumento11 pagineSurgical Specialties DR - PaghubasanRoyce Vincent TizonNessuna valutazione finora
- 16-Genital ProlapseDocumento37 pagine16-Genital Prolapseapi-3703352Nessuna valutazione finora
- Pancreas Pancreatic DisordersDocumento48 paginePancreas Pancreatic DisordersAmjad NiaziNessuna valutazione finora
- Acute PancreatitisDocumento46 pagineAcute PancreatitisLew NianNessuna valutazione finora
- Hepatobiliary DiseaseDocumento60 pagineHepatobiliary DiseaseFirdaus AslamNessuna valutazione finora
- 10 EdemaDocumento23 pagine10 EdemaTalmaciu AmyNessuna valutazione finora
- Benign Ovarian MassDocumento39 pagineBenign Ovarian MassVidhi Chaudhary100% (1)
- Neonatal Intestinal Obstruction EPSGHAN PDFDocumento77 pagineNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNessuna valutazione finora
- Intestinal Atresia and StenosisDocumento7 pagineIntestinal Atresia and StenosisMichael NafarinNessuna valutazione finora
- Abdominal Trauma Diagnosis and ClassificationDocumento129 pagineAbdominal Trauma Diagnosis and ClassificationTan DanNessuna valutazione finora
- The Abdominal OrgansDocumento56 pagineThe Abdominal OrgansAjeng FikihNessuna valutazione finora
- Pediatric Surgery Dr. A. IgamaDocumento6 paginePediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNessuna valutazione finora
- Ovarian CystsDocumento28 pagineOvarian CystsMuhammad AbeeshNessuna valutazione finora
- Image Interpretation 4Documento93 pagineImage Interpretation 4NanaJaeNessuna valutazione finora
- Male GU ExamDocumento5 pagineMale GU ExamOmar Farid ElgebalyNessuna valutazione finora
- Anorectal Anatomy & Surgical ManagementDocumento164 pagineAnorectal Anatomy & Surgical Managementsgod34Nessuna valutazione finora
- Development of MesentryDocumento28 pagineDevelopment of MesentryimmmiNessuna valutazione finora
- Genital ProlapseDocumento9 pagineGenital Prolapsesher singhNessuna valutazione finora
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocumento14 paginePaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanNessuna valutazione finora
- Hepatobiliary SystemDocumento18 pagineHepatobiliary SystemBinita ShresthaNessuna valutazione finora
- FLUIDS AND ELECTROLYTES MNGTDocumento44 pagineFLUIDS AND ELECTROLYTES MNGTremerose100% (1)
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocumento28 pagineOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNessuna valutazione finora
- Anatomia Peretelui AbdominalDocumento113 pagineAnatomia Peretelui Abdominalpandrea diana100% (1)
- A Disease Study On: AppendectomyDocumento8 pagineA Disease Study On: Appendectomybryan leguiabNessuna valutazione finora
- Anatomy of PeritoneumDocumento61 pagineAnatomy of PeritoneumFirdaus SeptiawanNessuna valutazione finora
- Gastrectomy 1Documento86 pagineGastrectomy 1Mysnow OpalNessuna valutazione finora
- Introduction To The Topographical Anatomy and Operative SurgeryDocumento43 pagineIntroduction To The Topographical Anatomy and Operative SurgeryKavan Vyas100% (1)
- Colon & Rectum Anatomy, Bleeding Causes, and Diagnosis ToolsDocumento186 pagineColon & Rectum Anatomy, Bleeding Causes, and Diagnosis ToolsMr AANessuna valutazione finora
- Direct Inguinal Hernia GuideDocumento11 pagineDirect Inguinal Hernia GuideRizka JamaraNessuna valutazione finora
- Dr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyDocumento55 pagineDr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyMohammad AliNessuna valutazione finora
- Benign Prostatic HypertrophyDocumento111 pagineBenign Prostatic HypertrophyOnkar SinghNessuna valutazione finora
- (Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Documento15 pagine(Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Aria Jean MostajoNessuna valutazione finora
- Abnormal Bowel Gas PatternDocumento136 pagineAbnormal Bowel Gas PatternEdward ElricNessuna valutazione finora
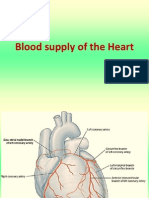
- Blood Supply of HeartDocumento7 pagineBlood Supply of Heartmariposa_0612Nessuna valutazione finora
- 17 - Gallbladder StonesDocumento71 pagine17 - Gallbladder StonesRashed ShatnawiNessuna valutazione finora
- Chronic Pelvic Pain Diagnosis and TreatmentDocumento48 pagineChronic Pelvic Pain Diagnosis and TreatmentFeruza SultanmuratovaNessuna valutazione finora
- Classes of AntibioticsDocumento7 pagineClasses of Antibioticsthoth_trismegistusNessuna valutazione finora
- SurgeryDocumento107 pagineSurgerymesenbetbuta21Nessuna valutazione finora
- Gastrointestinal and HepatobiliaryDocumento54 pagineGastrointestinal and Hepatobiliaryjeshema100% (1)
- Anatomy of the Pelvis and PerineumDocumento101 pagineAnatomy of the Pelvis and PerineumCiprianTeodorulNessuna valutazione finora
- Lymphatic SystemDocumento29 pagineLymphatic SystemlecturioNessuna valutazione finora
- Anatomy of Thyroid GlandDocumento12 pagineAnatomy of Thyroid GlandBinbinbabu BinuNessuna valutazione finora
- Neo BladderDocumento32 pagineNeo Bladderbelieveme030589Nessuna valutazione finora
- Surgical Female Urogenital Anatomy - UpToDateDocumento57 pagineSurgical Female Urogenital Anatomy - UpToDateErickNessuna valutazione finora
- Anatomy of BladderDocumento10 pagineAnatomy of BladderKiran tyraNessuna valutazione finora
- 54.the Gallbladder and Bile DuctsDocumento19 pagine54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondNessuna valutazione finora
- Bile Duct InjuryDocumento21 pagineBile Duct InjuryParul VarshneyNessuna valutazione finora
- Pancreatic Pseudocyst 2Documento37 paginePancreatic Pseudocyst 2AzharUlHassanQureshi100% (1)
- Fever and HyperthermiaDocumento6 pagineFever and HyperthermiaMarco Paulo Reyes NaoeNessuna valutazione finora
- Physiology Index CardsDocumento30 paginePhysiology Index CardsMarco Paulo Reyes NaoeNessuna valutazione finora
- Assessment of Back Pain-BMJDocumento30 pagineAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNessuna valutazione finora
- APRIL 2017: Aurora Hill and Engineer's Hill Health CentersDocumento2 pagineAPRIL 2017: Aurora Hill and Engineer's Hill Health CentersMarco Paulo Reyes NaoeNessuna valutazione finora
- Williams Endocrinology Large CoverDocumento1 paginaWilliams Endocrinology Large CoverMarco Paulo Reyes Naoe33% (9)
- SEIZURE CASE PROTOCOLDocumento1 paginaSEIZURE CASE PROTOCOLMarco Paulo Reyes NaoeNessuna valutazione finora
- Electronic Chapter Harrison's 19th EditionDocumento1 paginaElectronic Chapter Harrison's 19th EditionMarco Paulo Reyes Naoe0% (1)
- Ob-Gyn Post Graduate Interns May-June 2017-2018Documento1 paginaOb-Gyn Post Graduate Interns May-June 2017-2018Marco Paulo Reyes NaoeNessuna valutazione finora
- Table of Contents Williams Endocrinology 13th EditionDocumento4 pagineTable of Contents Williams Endocrinology 13th EditionMarco Paulo Reyes NaoeNessuna valutazione finora
- Gradeschool ReviewerDocumento7 pagineGradeschool ReviewerMarco Paulo Reyes NaoeNessuna valutazione finora
- Pharma Super TableDocumento56 paginePharma Super TableMarco Paulo Reyes NaoeNessuna valutazione finora
- Alcoholic Liver DiseaseDocumento22 pagineAlcoholic Liver DiseaseVikramjeet SinghNessuna valutazione finora
- Price List For PVC Single Loop Wire From OREZADocumento1 paginaPrice List For PVC Single Loop Wire From OREZAMarco Paulo Reyes NaoeNessuna valutazione finora
- CPC NarrationDocumento5 pagineCPC NarrationMarco Paulo Reyes NaoeNessuna valutazione finora
- Florist ContractDocumento1 paginaFlorist ContractMarco Paulo Reyes NaoeNessuna valutazione finora
- Special Awards - ListDocumento7 pagineSpecial Awards - ListMarco Paulo Reyes NaoeNessuna valutazione finora
- Liver Cirrhosis2 LectureDocumento104 pagineLiver Cirrhosis2 LectureMarco Paulo Reyes NaoeNessuna valutazione finora
- Approach to Leg Edema DiagnosisDocumento4 pagineApproach to Leg Edema DiagnosisMarco Paulo Reyes NaoeNessuna valutazione finora
- Selective Serotonin Reuptake Inhibitors: Naoe, Marco Paulo RDocumento38 pagineSelective Serotonin Reuptake Inhibitors: Naoe, Marco Paulo RMarco Paulo Reyes NaoeNessuna valutazione finora
- Pharma AntidiarrhealDocumento3 paginePharma AntidiarrhealMarco Paulo Reyes NaoeNessuna valutazione finora
- CPC SCRIPT SemifinalDocumento5 pagineCPC SCRIPT SemifinalMarco Paulo Reyes NaoeNessuna valutazione finora
- Admiting Conference - Acute GastroenteritisDocumento38 pagineAdmiting Conference - Acute GastroenteritisMarco Paulo Reyes NaoeNessuna valutazione finora
- The ParturientDocumento22 pagineThe ParturientMarco Paulo Reyes NaoeNessuna valutazione finora
- Pharma AntidiarrhealDocumento3 paginePharma AntidiarrhealMarco Paulo Reyes NaoeNessuna valutazione finora
- Acute Nephritic SyndromeDocumento1 paginaAcute Nephritic SyndromeMarco Paulo Reyes NaoeNessuna valutazione finora
- Adrenal Glands: I. Historical BackgroundDocumento7 pagineAdrenal Glands: I. Historical BackgroundMarco Paulo Reyes NaoeNessuna valutazione finora
- Cancer Drugs MRSDocumento12 pagineCancer Drugs MRSMarco Paulo Reyes NaoeNessuna valutazione finora
- Consent in Emergency CasesDocumento10 pagineConsent in Emergency CasesMarco Paulo Reyes NaoeNessuna valutazione finora
- 3rd and 4th Stage of Labor Dr. BaduaDocumento8 pagine3rd and 4th Stage of Labor Dr. BaduaMarco Paulo Reyes NaoeNessuna valutazione finora
- HISTOLO Lecture 4 - Histology of The Digestive SystemDocumento37 pagineHISTOLO Lecture 4 - Histology of The Digestive SystemResty De Guzman SoteloNessuna valutazione finora
- Liver Pancreas SpleenDocumento88 pagineLiver Pancreas SpleenGabi NaeNessuna valutazione finora
- Digestive SystemDocumento20 pagineDigestive SystemJerilee SoCute WattsNessuna valutazione finora
- Liver Healing 101 - Medical Medium ProtocolsDocumento10 pagineLiver Healing 101 - Medical Medium ProtocolsNina_C_AL93% (27)
- pubmed-FattyLiver-set 2Documento168 paginepubmed-FattyLiver-set 2marizaNessuna valutazione finora
- Digestive System (Unit X)Documento44 pagineDigestive System (Unit X)zahraNessuna valutazione finora
- Alcoholic HepatitisDocumento28 pagineAlcoholic HepatitisWaqar AhmedNessuna valutazione finora
- Neutrosec PPT BriefDocumento6 pagineNeutrosec PPT BriefBenNessuna valutazione finora
- Preface and Table of Contents - WordDocumento18 paginePreface and Table of Contents - WordAashima BhallaNessuna valutazione finora
- Abdominal Ultrasound - LiverDocumento30 pagineAbdominal Ultrasound - Liverpunct_org3256Nessuna valutazione finora
- Hepatic EncephalopathyDocumento16 pagineHepatic Encephalopathyjh_ajjNessuna valutazione finora
- Regulation of Organic Metabolism and Energy Balance: Multiple Choice QuestionsDocumento30 pagineRegulation of Organic Metabolism and Energy Balance: Multiple Choice QuestionswanderagroNessuna valutazione finora
- Guide Urine Therapy PDFDocumento12 pagineGuide Urine Therapy PDFMyland SaguNessuna valutazione finora
- The Mark of Athena2Documento10 pagineThe Mark of Athena2srasrk11Nessuna valutazione finora
- Case-Study VincentDocumento16 pagineCase-Study VincentKyle Audrie ArcalasNessuna valutazione finora
- Tokyo Guidelines 2018 - Surgical Management of Acute Cholecystitis - Safe Steps in Laparoscopic Cholecystectomy For Acute Cholecystitis (With Videos)Documento28 pagineTokyo Guidelines 2018 - Surgical Management of Acute Cholecystitis - Safe Steps in Laparoscopic Cholecystectomy For Acute Cholecystitis (With Videos)Karen Guerrero100% (1)
- Alcoholic Hepatitis: A ReviewDocumento9 pagineAlcoholic Hepatitis: A ReviewTugasbu CicikNessuna valutazione finora
- Ijbpr: International Journal of Biological & Pharmaceutical ResearchDocumento6 pagineIjbpr: International Journal of Biological & Pharmaceutical ResearchPharmaIntelligenceNessuna valutazione finora
- Full Autopsy Released in Death of Kyler PresnellDocumento9 pagineFull Autopsy Released in Death of Kyler PresnellKrystyna May67% (3)
- Frog Embryo Germ Layer DevelopmentDocumento10 pagineFrog Embryo Germ Layer DevelopmentJervis PendletonNessuna valutazione finora
- Gall StonesDocumento13 pagineGall StonesAdwaitha KrNessuna valutazione finora
- Liver Transplantation: What Is Liver Transplantation? Who Needs A Liver Transplant?Documento12 pagineLiver Transplantation: What Is Liver Transplantation? Who Needs A Liver Transplant?RatihSeptianiNessuna valutazione finora
- Lab Report NewDocumento2 pagineLab Report Newmohitsharma.jalNessuna valutazione finora