Potrebbero piacerti anche
- Motion To DismissDocumento24 pagineMotion To DismisssandyemerNessuna valutazione finora
- Comprehensive Handbook Obstetrics & Gynecology 3rd EdDa EverandComprehensive Handbook Obstetrics & Gynecology 3rd EdValutazione: 5 su 5 stelle5/5 (1)
- How To Guide To Oauth and API SecurityDocumento12 pagineHow To Guide To Oauth and API Securitysilviuleahu100% (1)
- Emergency Communication Procedures Communication Equipment Wake TurbulenceDocumento38 pagineEmergency Communication Procedures Communication Equipment Wake TurbulenceRaluca StoicaNessuna valutazione finora
- Proforma For Registration of Subject For Dissertation: Obstetrics and Gynecological NursingDocumento22 pagineProforma For Registration of Subject For Dissertation: Obstetrics and Gynecological Nursingrevathidadam55555Nessuna valutazione finora
- Filcar vs. EspinasDocumento2 pagineFilcar vs. EspinasBrian ThunderNessuna valutazione finora
- Too Much Time in Social Media and Its Effects On The 2nd Year BSIT Students of USTPDocumento48 pagineToo Much Time in Social Media and Its Effects On The 2nd Year BSIT Students of USTPLiam FabelaNessuna valutazione finora
- HANA Heroes 1 - EWM Lessons Learned (V2)Documento40 pagineHANA Heroes 1 - EWM Lessons Learned (V2)Larissa MaiaNessuna valutazione finora
- DX225LCA DX340LCA Sales MaterialDocumento46 pagineDX225LCA DX340LCA Sales MaterialAntonio Carrion100% (9)
- Rajiv Gandhi University of Health Sciences Karnataka, BangaloreDocumento22 pagineRajiv Gandhi University of Health Sciences Karnataka, BangaloreSadam HussienNessuna valutazione finora
- Goat Farm ProjectDocumento44 pagineGoat Farm ProjectVipin Kushwaha83% (6)
- Organisational Structure of NetflixDocumento2 pagineOrganisational Structure of NetflixAnkita Das57% (7)
- Rajiv Gandhi University of Health Sciences, Karnataka, BangaloreDocumento27 pagineRajiv Gandhi University of Health Sciences, Karnataka, BangaloreJyotiNessuna valutazione finora
- Effecttivenness of Birthball Usage During Labour On Pain and Child Birth Experience Among Primi Parturient Mothers: A Randomized Interventional StudyDocumento4 pagineEffecttivenness of Birthball Usage During Labour On Pain and Child Birth Experience Among Primi Parturient Mothers: A Randomized Interventional StudyShubhra PaulNessuna valutazione finora
- Monika SynopsisDocumento26 pagineMonika SynopsismahaNessuna valutazione finora
- A Comparative Study On Effect of Ambulation and Birthing Ball On Maternal and Newborn Outcome Among Primigravida Mothers in Selected Hospitals in MangalorDocumento4 pagineA Comparative Study On Effect of Ambulation and Birthing Ball On Maternal and Newborn Outcome Among Primigravida Mothers in Selected Hospitals in MangalorHella WarnierNessuna valutazione finora
- Maternal and Foetal Outcome of Single Dose Spinal Analgesia For Labour PainsDocumento3 pagineMaternal and Foetal Outcome of Single Dose Spinal Analgesia For Labour PainsGurnaman SinghNessuna valutazione finora
- Research SynopsisDocumento30 pagineResearch SynopsisAGERI PUSHPALATHANessuna valutazione finora
- PaaaaaaaaaaaaaaaaaaaaaaDocumento8 paginePaaaaaaaaaaaaaaaaaaaaaaByArdieNessuna valutazione finora
- Effect of Pregnancy Exercise On Duration of The First and Second Stage of Labor in Primigravida Mothers During The Third Trimester of PregnancyDocumento11 pagineEffect of Pregnancy Exercise On Duration of The First and Second Stage of Labor in Primigravida Mothers During The Third Trimester of Pregnancyoktavia mandaaNessuna valutazione finora
- Sri+Wahyuni+Bahrum Imelda BaruDocumento6 pagineSri+Wahyuni+Bahrum Imelda BaruWinda PuspitasariNessuna valutazione finora
- Maternal Positions and Mobility During First Stage LabourDocumento33 pagineMaternal Positions and Mobility During First Stage LabourdenisNessuna valutazione finora
- 24Documento7 pagine24Arti NegiNessuna valutazione finora
- Hartati 2019 J. Phys. Conf. Ser. 1351 012091Documento7 pagineHartati 2019 J. Phys. Conf. Ser. 1351 012091Derison MarsinovaNessuna valutazione finora
- Effects of Hydrotherapy During Labor Research Paper-2Documento11 pagineEffects of Hydrotherapy During Labor Research Paper-2api-597683251Nessuna valutazione finora
- Minor AilmentsDocumento14 pagineMinor AilmentsGazala100% (1)
- Proforma For Registration of Subject For DissertationDocumento27 pagineProforma For Registration of Subject For DissertationPriyanka Vikas TakNessuna valutazione finora
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocumento14 pagineRajiv Gandhi University of Health Sciences Bangalore, KarnatakaVeni SafitriNessuna valutazione finora
- Bangalore.: 1. Name of The Candidate and AddressDocumento21 pagineBangalore.: 1. Name of The Candidate and AddressHanny Novianti100% (2)
- Proforma For Registration of Subjects For DissertationDocumento15 pagineProforma For Registration of Subjects For DissertationQudrat Un NissaNessuna valutazione finora
- Effect of Dance Labor On The Management of Active Phase Labor Pain & Clients' Satisfaction: A Randomized Controlled Trial StudyDocumento9 pagineEffect of Dance Labor On The Management of Active Phase Labor Pain & Clients' Satisfaction: A Randomized Controlled Trial StudymfhfhfNessuna valutazione finora
- Oxytocin MassaseDocumento8 pagineOxytocin MassaseJery PradilaNessuna valutazione finora
- Childbirth in Supported Sitting Maternal PositionDocumento6 pagineChildbirth in Supported Sitting Maternal PositionLuisBarataGomesNessuna valutazione finora
- IJNER - 597 - 27 07 2018 Paper - R - 21Documento7 pagineIJNER - 597 - 27 07 2018 Paper - R - 21Yuning tyas Nursyah FitriNessuna valutazione finora
- Persistent Lateral and Posterior Fetal Positions at The Onset of Labour - 3 PDFDocumento7 paginePersistent Lateral and Posterior Fetal Positions at The Onset of Labour - 3 PDFOshigitaNessuna valutazione finora
- Dhana Final - 230915 - 104914Documento10 pagineDhana Final - 230915 - 104914JohnSundarNessuna valutazione finora
- Hubungan Posisi Mengejan Telentang Dan Kombinasi Dengan Lama Kala IiDocumento8 pagineHubungan Posisi Mengejan Telentang Dan Kombinasi Dengan Lama Kala IiNur muhardianaNessuna valutazione finora
- Jurnal Latihan Kegel ExcerciseDocumento6 pagineJurnal Latihan Kegel ExcerciseIksan KhoironiNessuna valutazione finora
- 7 Jurnal Dalam IngDocumento3 pagine7 Jurnal Dalam IngYeni terryNessuna valutazione finora
- JINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioDocumento13 pagineJINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioJashtine JingcoNessuna valutazione finora
- Correlation Between Menstrual Spasm and Labor ContractionDocumento7 pagineCorrelation Between Menstrual Spasm and Labor ContractionrvsharmaNessuna valutazione finora
- Vinita Jhariya: E-ISSN: 2664-2301 P-ISSN: 2664-2298Documento3 pagineVinita Jhariya: E-ISSN: 2664-2301 P-ISSN: 2664-2298Savita HanamsagarNessuna valutazione finora
- Analisis Faktor-Faktor Yang Berhubungan Dengan Pelaksanaan Senam Hamil Di Wilayah Puskesmas Purwokerto Barat Tahun 2013Documento9 pagineAnalisis Faktor-Faktor Yang Berhubungan Dengan Pelaksanaan Senam Hamil Di Wilayah Puskesmas Purwokerto Barat Tahun 2013Ferly OktriyediNessuna valutazione finora
- A Clinical Study of Programmed Labour and Its Maternal and Foetal OutcomeDocumento4 pagineA Clinical Study of Programmed Labour and Its Maternal and Foetal OutcomeInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Jurnal Posisi Kala II PartusDocumento10 pagineJurnal Posisi Kala II Partusichsan gamingNessuna valutazione finora
- A Study To Assess Effect of San-Yin-Jiao (SP-6) Acupressure On After Pains Among Multi Parous Women in A Selected Hospital in MangaloreDocumento6 pagineA Study To Assess Effect of San-Yin-Jiao (SP-6) Acupressure On After Pains Among Multi Parous Women in A Selected Hospital in MangaloreInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Painless Wit EpiduralDocumento7 paginePainless Wit Epiduralirvan rahmanNessuna valutazione finora
- Kaloji Narayana Rao University of Health and Science, Warangal, Telangana. Proforma For The Submission of SynopsisDocumento28 pagineKaloji Narayana Rao University of Health and Science, Warangal, Telangana. Proforma For The Submission of Synopsissaleha sultanaNessuna valutazione finora
- CD003934 AbstractDocumento3 pagineCD003934 AbstractLilik AnggrainiNessuna valutazione finora
- Birthing Ball Therapy in Labour To Reduce PainDocumento10 pagineBirthing Ball Therapy in Labour To Reduce PainSwapna Rajesh100% (1)
- Effect of Back Massage On Lactation Amon PDFDocumento9 pagineEffect of Back Massage On Lactation Amon PDFfemyNessuna valutazione finora
- Massagem Perineal em Trabalho de Parto e Prevenção de Trauma Perineal Ensaio Clínico RandomizadoDocumento4 pagineMassagem Perineal em Trabalho de Parto e Prevenção de Trauma Perineal Ensaio Clínico RandomizadoSheila SilvaNessuna valutazione finora
- O Gfshds Jjjp4Documento12 pagineO Gfshds Jjjp4BentaigaNessuna valutazione finora
- Chapter 6Documento5 pagineChapter 6k.s.newjin jamesNessuna valutazione finora
- Falla en Induccion de Trabajo de PartoDocumento9 pagineFalla en Induccion de Trabajo de PartoEliel MarcanoNessuna valutazione finora
- Prolonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)Documento5 pagineProlonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)siska tiaraNessuna valutazione finora
- AmniotomiDocumento8 pagineAmniotomibidan22Nessuna valutazione finora
- Proforma For Registration of Subject For: DissertationDocumento24 pagineProforma For Registration of Subject For: DissertationMALIK MANASRAHNessuna valutazione finora
- Effect of Acupressure On Nausea and Vomiting During PregnancyDocumento7 pagineEffect of Acupressure On Nausea and Vomiting During PregnancyArumDesiPratiwiNessuna valutazione finora
- Does Exercise Training During Pregnancy Affect Gestational Age? A Randomised Controlled TrialDocumento6 pagineDoes Exercise Training During Pregnancy Affect Gestational Age? A Randomised Controlled TrialTrnidad Moder GarvizoNessuna valutazione finora
- Knee Chest Position To Reduce The Incidence of Breech PresentationDocumento5 pagineKnee Chest Position To Reduce The Incidence of Breech PresentationNoviaNessuna valutazione finora
- Neetu, Poonam Sheoran, Rashmi PanchalDocumento6 pagineNeetu, Poonam Sheoran, Rashmi PanchalMuzdalifah Karina DMNessuna valutazione finora
- Experiences of Exercise During PregnancyDocumento9 pagineExperiences of Exercise During PregnancyNuno RobertoNessuna valutazione finora
- Journal Reading (LRDR)Documento2 pagineJournal Reading (LRDR)Andrea Albester GarinoNessuna valutazione finora
- VaughncapstonefinaldraftDocumento8 pagineVaughncapstonefinaldraftapi-356446630Nessuna valutazione finora
- 05 N141 31673Documento21 pagine05 N141 31673priya thakurNessuna valutazione finora
- 21Documento7 pagine21Sandy ApriNessuna valutazione finora
- Contoh Skenario - TelaahDocumento18 pagineContoh Skenario - TelaahnafiraNessuna valutazione finora
- Principles and Practice of UrogynaecologyDa EverandPrinciples and Practice of UrogynaecologyA TamilselviNessuna valutazione finora
- In Coming MailDocumento4 pagineIn Coming Mailpoetoet100% (1)
- What Is Bitcoin MiningDocumento4 pagineWhat Is Bitcoin MiningCarmen M Leal CurielNessuna valutazione finora
- Oxford Handbooks Online: From Old To New Developmentalism in Latin AmericaDocumento27 pagineOxford Handbooks Online: From Old To New Developmentalism in Latin AmericadiegoNessuna valutazione finora
- MTBE - Module - 3Documento83 pagineMTBE - Module - 3ABHIJITH V SNessuna valutazione finora
- Ljubljana European Green Capital 2016Documento56 pagineLjubljana European Green Capital 2016Kann_dandy17Nessuna valutazione finora
- Past Simple and Continuous - When - While Worksheet - Live WorksheetsDocumento4 paginePast Simple and Continuous - When - While Worksheet - Live WorksheetsSaraí CaracúnNessuna valutazione finora
- COMPLAINT - THE STAN J. CATERBONE 42 U.S.C. 14141 "POLICE MISCONDUCT PROVISION" COMPLAINT TO U.S. DEPARTMENT OF JUSTICE August 24, 2017Documento435 pagineCOMPLAINT - THE STAN J. CATERBONE 42 U.S.C. 14141 "POLICE MISCONDUCT PROVISION" COMPLAINT TO U.S. DEPARTMENT OF JUSTICE August 24, 2017Stan J. CaterboneNessuna valutazione finora
- How To Configure VFD - General - Guides & How-Tos - CoreELEC ForumsDocumento13 pagineHow To Configure VFD - General - Guides & How-Tos - CoreELEC ForumsJemerald MagtanongNessuna valutazione finora
- წყალტუბოს - სპა კურორტის განვითარების გეგმაDocumento16 pagineწყალტუბოს - სპა კურორტის განვითარების გეგმაReginfoNessuna valutazione finora
- Energy Facts PDFDocumento18 pagineEnergy Facts PDFvikas pandeyNessuna valutazione finora
- Definition of Sustainable Packaging PDFDocumento10 pagineDefinition of Sustainable Packaging PDFProf C.S.PurushothamanNessuna valutazione finora
- AutoCAD Civil 3D Performance Optimization 2Documento5 pagineAutoCAD Civil 3D Performance Optimization 2Renukadevi RptNessuna valutazione finora
- CH7Documento34 pagineCH7Abdul AzizNessuna valutazione finora
- Group9 SecADocumento7 pagineGroup9 SecAshivendrakadamNessuna valutazione finora
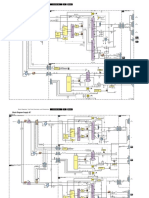
- Philips Chassis Lc4.31e Aa Power Dps 181 PDFDocumento9 paginePhilips Chassis Lc4.31e Aa Power Dps 181 PDFAouadi AbdellazizNessuna valutazione finora
- Poverty Eradication Cluster HLPF Position Paper With Case StudiesDocumento4 paginePoverty Eradication Cluster HLPF Position Paper With Case StudiesJohn Paul Demonteverde ElepNessuna valutazione finora
- Agenda 9Documento46 pagineAgenda 9Bala Gangadhar TilakNessuna valutazione finora
- Business Works Student User GuideDocumento14 pagineBusiness Works Student User GuideAkram UddinNessuna valutazione finora
- Vitus Bering, Centre For Higher Education: Jens Bertelsen & Jens Peder PedersenDocumento50 pagineVitus Bering, Centre For Higher Education: Jens Bertelsen & Jens Peder PedersenAnca IscruNessuna valutazione finora
- PETRO TCS Engineering Manual 682Documento44 paginePETRO TCS Engineering Manual 682paulm3565Nessuna valutazione finora
- KINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25Documento329 pagineKINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25http://secwatch.comNessuna valutazione finora