Potrebbero piacerti anche
- Medical Tribune February 2013 PHDocumento50 pagineMedical Tribune February 2013 PHPJHGNessuna valutazione finora
- Orthopedic Secrets, 3rd EditionDocumento61 pagineOrthopedic Secrets, 3rd EditionPJHG100% (10)
- Reflex Testing Method For Evaluating CNS DevelopmentDocumento55 pagineReflex Testing Method For Evaluating CNS DevelopmentPJHG100% (6)
- Medscape Complete Ruptures of The Achilles TendonDocumento27 pagineMedscape Complete Ruptures of The Achilles TendonPJHGNessuna valutazione finora
- Achilles Tendon Rupture 03Documento4 pagineAchilles Tendon Rupture 03PJHGNessuna valutazione finora
- 2008 Case Files AnatomyDocumento4 pagine2008 Case Files AnatomyPJHGNessuna valutazione finora
- 2007 Current Diagnosis & Treatment in Sports MedicineDocumento3 pagine2007 Current Diagnosis & Treatment in Sports MedicinePJHGNessuna valutazione finora
- PT OT Board Exam Result August 2012Documento11 paginePT OT Board Exam Result August 2012PJHGNessuna valutazione finora
- PRC PT Licensure Exam February 2012 List of PassersDocumento5 paginePRC PT Licensure Exam February 2012 List of PassersPJHGNessuna valutazione finora
- 2010 Schwartz's Principles of SurgeryDocumento4 pagine2010 Schwartz's Principles of SurgeryPJHG50% (2)
- Achilles Tendon Rupture 04Documento2 pagineAchilles Tendon Rupture 04PJHGNessuna valutazione finora
- Achilles Tendon Rupture 02Documento2 pagineAchilles Tendon Rupture 02PJHGNessuna valutazione finora
- 2010 A Guide To Sports InjuryDocumento2 pagine2010 A Guide To Sports InjuryPJHGNessuna valutazione finora
- Achilles Tendon Rupture 05Documento3 pagineAchilles Tendon Rupture 05PJHGNessuna valutazione finora
- 2007 Therapeutic Exercise Foundations and TechniquesDocumento8 pagine2007 Therapeutic Exercise Foundations and TechniquesPJHGNessuna valutazione finora
- Mri GlossaryDocumento12 pagineMri GlossaryPJHGNessuna valutazione finora
- Med Surge 06 OsteoarthritisDocumento2 pagineMed Surge 06 OsteoarthritisPJHGNessuna valutazione finora
- Achilles Tendon Rupture 01Documento1 paginaAchilles Tendon Rupture 01PJHGNessuna valutazione finora
- FLV To Mp3 File ConvertDocumento7 pagineFLV To Mp3 File ConvertPJHGNessuna valutazione finora
- Med Surge 02 Adhesive CapsulitisDocumento5 pagineMed Surge 02 Adhesive CapsulitisPJHGNessuna valutazione finora
- Med Surge 03 Rotator Cuff DisorderDocumento18 pagineMed Surge 03 Rotator Cuff DisorderPJHGNessuna valutazione finora
- Med Surge 05 Rheumatoid ArthritisDocumento3 pagineMed Surge 05 Rheumatoid ArthritisPJHGNessuna valutazione finora
- Med Surge 01 ScoliosisDocumento6 pagineMed Surge 01 ScoliosisPJHGNessuna valutazione finora
- Med Surge 04 Low Back PainDocumento6 pagineMed Surge 04 Low Back PainPJHGNessuna valutazione finora
- Integumentary System LATESTDocumento19 pagineIntegumentary System LATESTPJHGNessuna valutazione finora
- Comparison of UMN & LMN SyndromesDocumento2 pagineComparison of UMN & LMN SyndromesPJHGNessuna valutazione finora
- Rheumatoid ArthritisDocumento15 pagineRheumatoid ArthritisPJHG100% (2)
- Med SurgeDocumento251 pagineMed SurgePJHGNessuna valutazione finora
- Integumentary System Harrisons Manual of MedicineDocumento3 pagineIntegumentary System Harrisons Manual of MedicinePJHGNessuna valutazione finora
- Integumentary System Pathology Implications For PTDocumento8 pagineIntegumentary System Pathology Implications For PTPJHGNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- IMRT - ACR - ASTRO GuidelinesDocumento11 pagineIMRT - ACR - ASTRO GuidelinesSayan DasNessuna valutazione finora
- Imaging of Chest DiseasesDocumento184 pagineImaging of Chest DiseasesGembong Putro100% (1)
- Genes and Cancer: Understanding the Role of Genetics in Cancer DevelopmentDocumento42 pagineGenes and Cancer: Understanding the Role of Genetics in Cancer DevelopmentAnes JogunčićNessuna valutazione finora
- Balance The Imbalance: Diagnosis & Management of Vertigo - PresentDocumento111 pagineBalance The Imbalance: Diagnosis & Management of Vertigo - PresentPraveen KumarNessuna valutazione finora
- LiliDocumento7 pagineLilialan azizNessuna valutazione finora
- Revlon Case StudyDocumento5 pagineRevlon Case StudyAriel Anthonie Puso GarciaNessuna valutazione finora
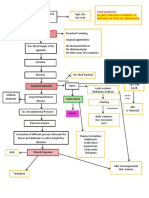
- CPC - Appendicitis (Flowchart)Documento1 paginaCPC - Appendicitis (Flowchart)Milet NacionalesNessuna valutazione finora
- Full RujiraLeukorrhea, STDS, HIV Infection.02102017 PDFDocumento129 pagineFull RujiraLeukorrhea, STDS, HIV Infection.02102017 PDFrujiraNessuna valutazione finora
- Expert Committee On The Diagnosis and Classification of Diabetes (2003) PDFDocumento16 pagineExpert Committee On The Diagnosis and Classification of Diabetes (2003) PDFPattyNessuna valutazione finora
- Human NutritionDocumento35 pagineHuman Nutritionriareyes86Nessuna valutazione finora
- Haamid2017 PDFDocumento25 pagineHaamid2017 PDFAhmad SyaukatNessuna valutazione finora
- Age Specific20060906Documento26 pagineAge Specific20060906Danily Faith VillarNessuna valutazione finora
- Deep Nutrition Why Your Genes Need Traditional FoodDocumento15 pagineDeep Nutrition Why Your Genes Need Traditional Foodk2057282100% (1)
- Sensory - Unit 1Documento45 pagineSensory - Unit 1AKASH SNessuna valutazione finora
- Kendler 2005Documento10 pagineKendler 2005MaximilianNessuna valutazione finora
- Serous Effusion and Synovial Fluid Visual Characteristics and Laboratory TestsDocumento4 pagineSerous Effusion and Synovial Fluid Visual Characteristics and Laboratory TestsstellaNessuna valutazione finora
- Serenoa Repens (Saw Palmetto) A Systematic Review of Adverse EventsDocumento11 pagineSerenoa Repens (Saw Palmetto) A Systematic Review of Adverse EventsAdam ZhangNessuna valutazione finora
- Reproductive System AnatomyDocumento30 pagineReproductive System AnatomyJune PinedaNessuna valutazione finora
- Herpes Simplex I and IIDocumento50 pagineHerpes Simplex I and IItummalapalli venkateswara raoNessuna valutazione finora
- Diagnostic Strategy in RheumatologyDocumento8 pagineDiagnostic Strategy in RheumatologyMadalina LucaNessuna valutazione finora
- Celiac DiseaseDocumento43 pagineCeliac DiseasefajarNessuna valutazione finora
- Cervical PolypDocumento3 pagineCervical PolypLiyona RifaniNessuna valutazione finora
- Current Therapy of Trauma and Surgical Critical CareDocumento4 pagineCurrent Therapy of Trauma and Surgical Critical CareAgung TananNessuna valutazione finora
- Stromberg Gross Path Text Handout AU DVP 2016Documento29 pagineStromberg Gross Path Text Handout AU DVP 2016Rachel Autran100% (1)
- Calmine-Hine 1995 Cancer ReportDocumento34 pagineCalmine-Hine 1995 Cancer ReportShirley SpenceNessuna valutazione finora
- 2008 04 Lecture 1 Interface Dermatitis FrishbergDocumento6 pagine2008 04 Lecture 1 Interface Dermatitis FrishbergYudistra R ShafarlyNessuna valutazione finora
- Diagnosis and Management of Tonsillitis GuidelineDocumento23 pagineDiagnosis and Management of Tonsillitis GuidelinemarcelinaNessuna valutazione finora
- Locomotor System Study GuideDocumento80 pagineLocomotor System Study Guidemartincorbacho100% (1)
- Neoplasia Outline Notes - PathologyDocumento4 pagineNeoplasia Outline Notes - Pathologykep1313Nessuna valutazione finora