Potrebbero piacerti anche
- High Yield Surgery Shelf ReviewDocumento77 pagineHigh Yield Surgery Shelf ReviewDuke71% (7)
- Adrenal Gland OSCEDocumento14 pagineAdrenal Gland OSCEOmar AttaNessuna valutazione finora
- Endocrine Disorders (Study Notes)Documento11 pagineEndocrine Disorders (Study Notes)Danelle Harrison, RN90% (10)
- Step-2-Ck-Notes-Syrian-Student - HTML: Cardiology UWDocumento15 pagineStep-2-Ck-Notes-Syrian-Student - HTML: Cardiology UWLoyla RoseNessuna valutazione finora
- Keto Supplement GuideDocumento10 pagineKeto Supplement Guideyesopunk67% (3)
- Nephrology - Dr. Allam 2021Documento42 pagineNephrology - Dr. Allam 2021Alokh Saha RajNessuna valutazione finora
- Surgery 2012Documento28 pagineSurgery 2012max_21ruNessuna valutazione finora
- Endocrinology Board Review: Thyroid DisordersDocumento46 pagineEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoNessuna valutazione finora
- USMLE Step 2 CK Notes on Neurology and Neurological ConditionsDocumento5 pagineUSMLE Step 2 CK Notes on Neurology and Neurological ConditionsLoyla RoseNessuna valutazione finora
- Cardiology Notes Syrian StudentDocumento10 pagineCardiology Notes Syrian Studentabuzeid5Nessuna valutazione finora
- Infections PDFDocumento40 pagineInfections PDFLoyla Rose100% (1)
- Harrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Documento707 pagineHarrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Choi DongYiNessuna valutazione finora
- Krisis HipertensiDocumento12 pagineKrisis HipertensiDani NurseNessuna valutazione finora
- Seiler Athletics Hierarchy of Training Needs Presentation-Revisedandannotated PDFDocumento79 pagineSeiler Athletics Hierarchy of Training Needs Presentation-Revisedandannotated PDFBLLYDNessuna valutazione finora
- USMLE Review Program Covers Steps 1, 2 and 3Documento1 paginaUSMLE Review Program Covers Steps 1, 2 and 3wldcrdNessuna valutazione finora
- Treatment of Resistant and Refractory HypertensionDocumento21 pagineTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- Neet PG 2021 Q&A Medical JunctionDocumento144 pagineNeet PG 2021 Q&A Medical JunctionKk bhaiNessuna valutazione finora
- Fitness - ACE Fitness Center - Circuit TrainingDocumento2 pagineFitness - ACE Fitness Center - Circuit TrainingdiegoNessuna valutazione finora
- 1 Drugs Affecting The Endocrine SystemDocumento61 pagine1 Drugs Affecting The Endocrine SystemHERLIN HOBAYANNessuna valutazione finora
- IM STEP 2 NotesDocumento74 pagineIM STEP 2 Notesyanks1120100% (3)
- Drugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Documento467 pagineDrugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Marc Imhotep Cray, M.D.100% (1)
- FlashcardsforStep2Part2 PDFDocumento12 pagineFlashcardsforStep2Part2 PDFLoyla RoseNessuna valutazione finora
- FlashcardsforStep2Part2 PDFDocumento12 pagineFlashcardsforStep2Part2 PDFLoyla RoseNessuna valutazione finora
- Alert Medical Series: Emergency Medicine Alert IIIDa EverandAlert Medical Series: Emergency Medicine Alert IIINessuna valutazione finora
- Amboss:CardioDocumento18 pagineAmboss:CardioNicole Juliette CCNessuna valutazione finora
- Hematology Oncology Notes Syrian StudentDocumento2 pagineHematology Oncology Notes Syrian StudentLoyla RoseNessuna valutazione finora
- USMLE Step 2 CK 6 Months Study Plan For 240Documento1 paginaUSMLE Step 2 CK 6 Months Study Plan For 240DhritisdiaryNessuna valutazione finora
- Occupational Health Hazards for Women in the Pharmaceutical IndustryDocumento61 pagineOccupational Health Hazards for Women in the Pharmaceutical IndustryCostas JacovidesNessuna valutazione finora
- Pediatrics 04: 8-Year-Old Male Well-Child Check: Learning ObjectivesDocumento8 paginePediatrics 04: 8-Year-Old Male Well-Child Check: Learning ObjectivesJeffNessuna valutazione finora
- 390 QuestionsDocumento26 pagine390 QuestionsBenie BudNessuna valutazione finora
- Flashcards For Step 2 Part 1Documento39 pagineFlashcards For Step 2 Part 1Loyla RoseNessuna valutazione finora
- Gastroenterology: Diseases of The EsophagusDocumento18 pagineGastroenterology: Diseases of The EsophagusKayeshiana30Nessuna valutazione finora
- Micro Biology: Pgei Golden Points 2015Documento27 pagineMicro Biology: Pgei Golden Points 2015Challa Krishna VasanNessuna valutazione finora
- Pathology Questions PDFDocumento67 paginePathology Questions PDFDhruva PatelNessuna valutazione finora
- 1992-1997 and 2004 Questions and AnswersDocumento56 pagine1992-1997 and 2004 Questions and AnswersEmad MerganNessuna valutazione finora
- 07 EndocrineDocumento44 pagine07 Endocrineandirio7486Nessuna valutazione finora
- Charles Poliquin How To Plan Your Workouts PDFDocumento2 pagineCharles Poliquin How To Plan Your Workouts PDFRajdeep Nath50% (2)
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- What Is Malnutrition?: WastingDocumento6 pagineWhat Is Malnutrition?: WastingĐoan VõNessuna valutazione finora
- Test CentreDocumento178 pagineTest CentreShaik Nizam Uddin100% (1)
- 2023 MayDocumento36 pagine2023 MayReshma Shaji PnsNessuna valutazione finora
- Endocrine HTNDocumento32 pagineEndocrine HTNatik mayasariNessuna valutazione finora
- Kaplan All SubjectsDocumento8 pagineKaplan All Subjectssarmad_bayatliNessuna valutazione finora
- Endocrine Disorders 1234399857677955 1Documento130 pagineEndocrine Disorders 1234399857677955 1api-19824701Nessuna valutazione finora
- Animals Rely On Two Systems For Regulation:: Nervous System Is A System of Nerve Cells Called Neurons. ItDocumento24 pagineAnimals Rely On Two Systems For Regulation:: Nervous System Is A System of Nerve Cells Called Neurons. It陳品汎Nessuna valutazione finora
- Banco Kap. - CK 2Documento1.099 pagineBanco Kap. - CK 2Lucas OrtizNessuna valutazione finora
- Laboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPDocumento41 pagineLaboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPmarieNessuna valutazione finora
- DR Saleh Course fainalSEPT 20Documento103 pagineDR Saleh Course fainalSEPT 20JehanzebNessuna valutazione finora
- AIR DROP EXAMنسختي PDFDocumento35 pagineAIR DROP EXAMنسختي PDFYara AlmouallemNessuna valutazione finora
- High Yield Topics For PhysiologyDocumento68 pagineHigh Yield Topics For PhysiologyTina De Leon YacatNessuna valutazione finora
- Blood and Drugs Medicine NotesDocumento39 pagineBlood and Drugs Medicine Notesrahuul prasadNessuna valutazione finora
- Nrtis: (Nucleoside/ Nucleotide Reverse Transcriptase) : "Eatz LSD"Documento3 pagineNrtis: (Nucleoside/ Nucleotide Reverse Transcriptase) : "Eatz LSD"Mohammad KatatoNessuna valutazione finora
- Aquifer InternalMedicine09 - 55Documento7 pagineAquifer InternalMedicine09 - 55JulieNessuna valutazione finora
- Acid - Base DisordersDocumento16 pagineAcid - Base DisordersPuteri PudingNessuna valutazione finora
- 571 FullDocumento2 pagine571 FullJauhari JoNessuna valutazione finora
- OBGYN HistoryDocumento1 paginaOBGYN Historysgod34Nessuna valutazione finora
- Hyper & Hypothyroidism LectureDocumento1 paginaHyper & Hypothyroidism LectureJhevilin RMNessuna valutazione finora
- GP Reg - Asthma and Spirometry 2011Documento114 pagineGP Reg - Asthma and Spirometry 2011minerva_stanciuNessuna valutazione finora
- Certifying DeathDocumento8 pagineCertifying DeathDaniel LimNessuna valutazione finora
- Preventive CardiologyDocumento28 paginePreventive CardiologyerizonNessuna valutazione finora
- Mock Record B-1-2-Well Child VisitsDocumento4 pagineMock Record B-1-2-Well Child VisitsaelteeNessuna valutazione finora
- UTIDocumento17 pagineUTIBongkotchakorn Mind PhonchaiNessuna valutazione finora
- History Taking OSCE Example 4Documento6 pagineHistory Taking OSCE Example 4worlddoctor2012Nessuna valutazione finora
- Pre Assessment Diabetes Nursing CareDocumento4 paginePre Assessment Diabetes Nursing CareHabib UllahNessuna valutazione finora
- 58 Cases History and Physical Exam BookDocumento102 pagine58 Cases History and Physical Exam BookeleazarmdNessuna valutazione finora
- Normal Laboratory Values With Nursing Consideration - UsnganDocumento8 pagineNormal Laboratory Values With Nursing Consideration - UsnganPrincess Nasima M. UsnganNessuna valutazione finora
- CNS Seizures in ChildhoodDocumento42 pagineCNS Seizures in ChildhoodDr.P.NatarajanNessuna valutazione finora
- Diagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia PDFDocumento14 pagineDiagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia PDFSurat Saengjinda100% (1)
- Aquifer InternalMedicine11 - 45Documento8 pagineAquifer InternalMedicine11 - 45JulieNessuna valutazione finora
- Thyroid DisordersDocumento21 pagineThyroid DisordersSuliman GarallehNessuna valutazione finora
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocumento8 pagineApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuNessuna valutazione finora
- Endocrine Case StudiesDocumento16 pagineEndocrine Case StudiesIdrissa John Sebeh Conteh0% (1)
- Lung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyDa EverandLung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyPhilip FarrellNessuna valutazione finora
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- Diseases of The Thyroid GlandDocumento3 pagineDiseases of The Thyroid GlandLoyla RoseNessuna valutazione finora
- Endocrin 5Documento6 pagineEndocrin 5Loyla RoseNessuna valutazione finora
- Rheumatology Notes Syrian StudentDocumento2 pagineRheumatology Notes Syrian StudentLoyla RoseNessuna valutazione finora
- Neurology Notes Syrian StudentDocumento5 pagineNeurology Notes Syrian StudentLiridon SopajNessuna valutazione finora
- Rheumatology: - Syrian - Notes - CK - 2 - Step - Usmle - Pieces/8806 - Bits - CK - 2 - Step - Student - HTMLDocumento5 pagineRheumatology: - Syrian - Notes - CK - 2 - Step - Usmle - Pieces/8806 - Bits - CK - 2 - Step - Student - HTMLLoyla RoseNessuna valutazione finora
- Gastroenterology notes for USMLE preparationDocumento2 pagineGastroenterology notes for USMLE preparationLoyla RoseNessuna valutazione finora
- Selling: Economics 100: Introduction To EconomicsDocumento19 pagineSelling: Economics 100: Introduction To EconomicsLoyla RoseNessuna valutazione finora
- Gynecology TableDocumento2 pagineGynecology TableLoyla RoseNessuna valutazione finora
- Epifeed LHFDocumento2 pagineEpifeed LHFJoko WiwiNessuna valutazione finora
- IDF Diabetes Atlas 2ndedDocumento297 pagineIDF Diabetes Atlas 2ndedatikdiyahNessuna valutazione finora
- 9.intracellular Accumulations 1Documento45 pagine9.intracellular Accumulations 1Ramesh KumarNessuna valutazione finora
- Daftar PustakaDocumento10 pagineDaftar PustakaShafiraNessuna valutazione finora
- Zumba - Guia en InglesDocumento32 pagineZumba - Guia en Inglesvskavo100% (1)
- Fatty Acids SynthesisDocumento30 pagineFatty Acids SynthesisGhaidaa SadeqNessuna valutazione finora
- Training Energy Systems Through IntervalsDocumento19 pagineTraining Energy Systems Through IntervalsIndu G MathiNessuna valutazione finora
- of Lipid Biocmeistry FinalDocumento25 pagineof Lipid Biocmeistry FinalInd-Wan Fatwindari PrasetyoNessuna valutazione finora
- Medical Nutrition Therapy For UnderweightDocumento2 pagineMedical Nutrition Therapy For UnderweightAkshaya KherNessuna valutazione finora
- 1 s2.0 S1056872722000071 MainDocumento5 pagine1 s2.0 S1056872722000071 Maindzaky fadhilNessuna valutazione finora
- JCC Membership Packages and Benefits for Families and IndividualsDocumento2 pagineJCC Membership Packages and Benefits for Families and IndividualsDiane YangNessuna valutazione finora
- Obesity Case StudyDocumento10 pagineObesity Case StudyPhavarasan ArasanNessuna valutazione finora
- Insuline IndexDocumento28 pagineInsuline IndexcasaberkaneNessuna valutazione finora
- Recommended Weight Gain During Pregnancy ForDocumento2 pagineRecommended Weight Gain During Pregnancy Forabdelhamed aliNessuna valutazione finora
- Resume of Tiffany LDocumento2 pagineResume of Tiffany Lapi-537156502Nessuna valutazione finora
- Perception of The Custumer Toward To The Food Restaurant To Be Built in Boac MarinduqueDocumento18 paginePerception of The Custumer Toward To The Food Restaurant To Be Built in Boac MarinduqueIshigami SenkuNessuna valutazione finora
- Medical CertificateDocumento2 pagineMedical CertificatelekacaNessuna valutazione finora
- Sepsis from UTI due to uncontrolled diabetesDocumento1 paginaSepsis from UTI due to uncontrolled diabetesJobelle Rodriguez BernabeNessuna valutazione finora
- Framework CVCBDocumento73 pagineFramework CVCBSiti Ika FitrasyahNessuna valutazione finora
- ULTIMATE CHEST Workout Plan by Guru MannDocumento4 pagineULTIMATE CHEST Workout Plan by Guru MannAman GuptaNessuna valutazione finora
- Farmakologi Benincasa Hispida (Kundur)Documento11 pagineFarmakologi Benincasa Hispida (Kundur)Syahrir ManaanNessuna valutazione finora
- Adolescent and Child Nutrition BasicsDocumento24 pagineAdolescent and Child Nutrition BasicsMike BoribsNessuna valutazione finora
- A1 Vs A2 Milk and Its SourceDocumento1 paginaA1 Vs A2 Milk and Its SourcecrneeteshNessuna valutazione finora
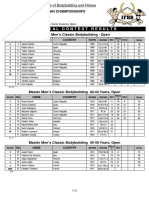
- 2019 Europeans ResultsDocumento12 pagine2019 Europeans Resultsxosmar185Nessuna valutazione finora