Potrebbero piacerti anche
- Falls: A Geriatric Syndrome: Jacqueline Jordan Lloyd, MD Florida State University College of MedicineDocumento15 pagineFalls: A Geriatric Syndrome: Jacqueline Jordan Lloyd, MD Florida State University College of MedicinePremaKurniaNessuna valutazione finora
- Section 1. Definition and Classification of Acute Kidney InjuryDocumento18 pagineSection 1. Definition and Classification of Acute Kidney InjuryPremaKurniaNessuna valutazione finora
- Intravenous Fluid Therapy For Adults in Hospital Clinical GuidelineDocumento10 pagineIntravenous Fluid Therapy For Adults in Hospital Clinical GuidelinePremaKurniaNessuna valutazione finora
- Roland Morris Low Back Pain and Disability Questionnaire rmq1 PDFDocumento2 pagineRoland Morris Low Back Pain and Disability Questionnaire rmq1 PDFPremaKurniaNessuna valutazione finora
- CHOLANGIOCARCINOMADocumento26 pagineCHOLANGIOCARCINOMAPremaKurnia100% (3)
- Cholangiocarcinoma Differential DiagnosisDocumento2 pagineCholangiocarcinoma Differential DiagnosisPremaKurniaNessuna valutazione finora
- Retinopathy of Prematurity Are Differentiated From Other Causes of Leukocoria. Most Important Differential Diagnosis IncludesDocumento2 pagineRetinopathy of Prematurity Are Differentiated From Other Causes of Leukocoria. Most Important Differential Diagnosis IncludesPremaKurniaNessuna valutazione finora
- Osteomyelitis in Long Bones: by Luca Lazzarini, Jon T. Mader, and Jason H. CalhounDocumento5 pagineOsteomyelitis in Long Bones: by Luca Lazzarini, Jon T. Mader, and Jason H. CalhounPremaKurniaNessuna valutazione finora
- Use of White Blood Cell Count and Negative Appendectomy RateDocumento8 pagineUse of White Blood Cell Count and Negative Appendectomy RatePremaKurniaNessuna valutazione finora
- De Quervain S TenosynovitisDocumento13 pagineDe Quervain S TenosynovitisPremaKurniaNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- January 2011 MS - Unit 1 Edexcel Biology A-LevelDocumento24 pagineJanuary 2011 MS - Unit 1 Edexcel Biology A-LevelAyse KerimNessuna valutazione finora
- Relacion Colesterol Total A HDL y Colesterol No HD PDFDocumento9 pagineRelacion Colesterol Total A HDL y Colesterol No HD PDFJoseAbdalaNessuna valutazione finora
- Cardiovascular System Abbas HayatDocumento35 pagineCardiovascular System Abbas HayatFiaz medicoNessuna valutazione finora
- Practical Cardiology An Approach To The Management of Problems in Cardiology (PDFDrive)Documento405 paginePractical Cardiology An Approach To The Management of Problems in Cardiology (PDFDrive)hendratj90Nessuna valutazione finora
- Alfonso Lopez CardiovascularDocumento15 pagineAlfonso Lopez Cardiovascularjaniceli0207Nessuna valutazione finora
- Coronary Artery Disease (Cad)Documento4 pagineCoronary Artery Disease (Cad)Freddy PanjaitanNessuna valutazione finora
- Percutaneous Transluminal Coronary AngioplastyDocumento22 paginePercutaneous Transluminal Coronary AngioplastyArya Gaunker100% (1)
- Case StudyDocumento63 pagineCase StudyRita PokharelNessuna valutazione finora
- Pathology of HEART - 1Documento175 paginePathology of HEART - 1Abdukadir AzamNessuna valutazione finora
- NCM 41118L Final Quiz 2Documento10 pagineNCM 41118L Final Quiz 2Matelyn OargaNessuna valutazione finora
- Cardiovascular Diseases: CVD's in The PhilippinesDocumento10 pagineCardiovascular Diseases: CVD's in The PhilippinesGellyace A.Nessuna valutazione finora
- Enzyme 20pagesDocumento20 pagineEnzyme 20pagesEddie Optin100% (2)
- Interpreting The Coronary-Artery Calcium ScoreDocumento3 pagineInterpreting The Coronary-Artery Calcium ScoreGaby Alejandra Ordonez AndradeNessuna valutazione finora
- MARK SCHEME For The June 2005 Question PaperDocumento10 pagineMARK SCHEME For The June 2005 Question PaperequatorloungeNessuna valutazione finora
- Coronary Artery DiseaseDocumento13 pagineCoronary Artery DiseaseChristianHanjokarNessuna valutazione finora
- Interventional CardiologyDocumento36 pagineInterventional CardiologyRufus RajNessuna valutazione finora
- Abstract Book INAACCDocumento83 pagineAbstract Book INAACCrodtobingNessuna valutazione finora
- Neclex Questions Test 3Documento16 pagineNeclex Questions Test 3Brittany Worrall100% (13)
- F1000research 7 16443Documento8 pagineF1000research 7 16443Muhammad AzamNessuna valutazione finora
- Patofisiologi Sistem KardiovaskularDocumento157 paginePatofisiologi Sistem KardiovaskularNyanmaruNessuna valutazione finora
- Pathology EssayDocumento19 paginePathology EssayARUNSKNessuna valutazione finora
- Peripheral Vascular InterventionsDocumento1.225 paginePeripheral Vascular InterventionsAvinash6614Nessuna valutazione finora
- Thesis On Coronary Heart DiseaseDocumento7 pagineThesis On Coronary Heart Diseasetracyclarkwarren100% (1)
- Case Study in NutritionDocumento27 pagineCase Study in NutritionTina TalmadgeNessuna valutazione finora
- Age-Related Impairment of Vascular Structure and FunctionsDocumento21 pagineAge-Related Impairment of Vascular Structure and FunctionsSomnis VeritasNessuna valutazione finora
- Hyperlipidemia in Diabetes-Etiology, Consequences and Treatment Edward Shahady MD Athero-Thrombosis in DiabetesDocumento6 pagineHyperlipidemia in Diabetes-Etiology, Consequences and Treatment Edward Shahady MD Athero-Thrombosis in DiabetesindahkurNessuna valutazione finora
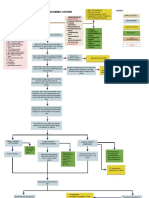
- Acute Ischemic Stroke Concept MapDocumento6 pagineAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Renal Artery Stenosis Treatment Consumer GuideDocumento8 pagineRenal Artery Stenosis Treatment Consumer GuideAHRQEHCProgramNessuna valutazione finora
- Biologic Crisis:: Prepared By: Recitas, Anna Lou G. BSN-4 Sn-DoscstDocumento64 pagineBiologic Crisis:: Prepared By: Recitas, Anna Lou G. BSN-4 Sn-DoscstDonna Solamo TalabocNessuna valutazione finora
- PHYS 3616E Chap91Documento15 paginePHYS 3616E Chap91johnNessuna valutazione finora