Potrebbero piacerti anche
- Toyota R150 R151Documento4 pagineToyota R150 R151Christian Rhadames Barkley Chavez100% (1)
- Pro StarDocumento263 paginePro StarLuis EduardoNessuna valutazione finora
- Fitness in The Extended Fascial ParadigmDocumento37 pagineFitness in The Extended Fascial Paradigmgavinbroomes100% (1)
- Functional Neuromuscular AnatomyDocumento56 pagineFunctional Neuromuscular AnatomyΒασίλης Βασιλείου100% (3)
- Does Fascia Hold Memories PDFDocumento7 pagineDoes Fascia Hold Memories PDFRandi Harvey100% (1)
- 32 Understanding Fibroblasts in Order To Comprehend The Osteopathic Treatment of The FasciaDocumento8 pagine32 Understanding Fibroblasts in Order To Comprehend The Osteopathic Treatment of The FasciaRenan O. Pravatta PivettaNessuna valutazione finora
- Bio Dynamics The Fascia of The Pelvic Floor Model of TensegrityDocumento8 pagineBio Dynamics The Fascia of The Pelvic Floor Model of TensegritygabrielsantosmsNessuna valutazione finora
- Uk QuizDocumento2 pagineUk QuizamcieqNessuna valutazione finora
- Visceral Manipulation in Structural Work: Liz Gaggini, M.ADocumento6 pagineVisceral Manipulation in Structural Work: Liz Gaggini, M.AleoNessuna valutazione finora
- Goering AAO Convocation2012LectureDocumento110 pagineGoering AAO Convocation2012Lectureperrolobo73Nessuna valutazione finora
- 2003 Fascial Mechanoreceptors and Their Potential Role in Deep Tissue ManipulationDocumento10 pagine2003 Fascial Mechanoreceptors and Their Potential Role in Deep Tissue Manipulation1RogerioNessuna valutazione finora
- The Compensatory Pattern As Seen in Art and OsteopathyDocumento3 pagineThe Compensatory Pattern As Seen in Art and OsteopathygelucNessuna valutazione finora
- Releasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueDa EverandReleasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueValutazione: 5 su 5 stelle5/5 (1)
- Double Rope TechniqueDocumento5 pagineDouble Rope TechniqueDougNewNessuna valutazione finora
- Unlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkDa EverandUnlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkNessuna valutazione finora
- Strength Training Using Myofascial LinesDocumento15 pagineStrength Training Using Myofascial LinesCris Cavasotto100% (1)
- ECS Training PDFDocumento193 pagineECS Training PDFAbdelhak Ezzahrioui100% (1)
- 2010 The Fascial Manipulation Technique and Its Biomechanical Model: A Guide To The Human Fascial SystemDocumento3 pagine2010 The Fascial Manipulation Technique and Its Biomechanical Model: A Guide To The Human Fascial System1Rogerio100% (1)
- Tom Myers Dynamic LigamentsDocumento4 pagineTom Myers Dynamic LigamentsAlisaClark100% (3)
- The Fascial System Is Sensory OrganDocumento6 pagineThe Fascial System Is Sensory OrganharmziieNessuna valutazione finora
- Visceral - Manipulation A Powerful New Frontier in BodyworkDocumento5 pagineVisceral - Manipulation A Powerful New Frontier in BodyworkDerek Kim100% (1)
- Fascial Manipulation Concepts and TechniquesDocumento6 pagineFascial Manipulation Concepts and Techniquestvbuddy123100% (1)
- Fascial Manipulations For Internal Pain PDFDocumento16 pagineFascial Manipulations For Internal Pain PDFdavidzhou0% (2)
- Fascia Forgotten StructureDocumento12 pagineFascia Forgotten StructureFraan GutierrezNessuna valutazione finora
- The Fascia The Forgotten Structure PDFDocumento12 pagineThe Fascia The Forgotten Structure PDFJorge100% (1)
- Workshop 1 PowerpointDocumento10 pagineWorkshop 1 PowerpointCarlos CorreaNessuna valutazione finora
- Cranial Osteopathy Its Fate Seems ClearDocumento3 pagineCranial Osteopathy Its Fate Seems ClearInvincy JYNessuna valutazione finora
- Lect Modalities - MET, HVLA, CSDocumento44 pagineLect Modalities - MET, HVLA, CSSean LeeNessuna valutazione finora
- The evolution of orthopaedic surgery and prosthesesDocumento244 pagineThe evolution of orthopaedic surgery and prosthesesMarisa Piazze83% (6)
- FasciaDocumento58 pagineFasciaMartín BiancalanaNessuna valutazione finora
- Fascia Book ReviewDocumento4 pagineFascia Book ReviewÁgnes LovasNessuna valutazione finora
- Kinetic ChainsDocumento5 pagineKinetic ChainsYermia RashaquatNessuna valutazione finora
- Fascia and Fascia Lines PDFDocumento7 pagineFascia and Fascia Lines PDFBeta LisboaNessuna valutazione finora
- Stecco Workshop Full TextDocumento18 pagineStecco Workshop Full TexthprieelsNessuna valutazione finora
- The Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1Documento9 pagineThe Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1nish0420100% (1)
- AAO FDM Indroduction 1994 PDFDocumento12 pagineAAO FDM Indroduction 1994 PDFHONGJYNessuna valutazione finora
- The Asymmetric Pelvis: Liz Gaggini, M.ADocumento7 pagineThe Asymmetric Pelvis: Liz Gaggini, M.Aleo100% (1)
- Muscle EnergyDocumento22 pagineMuscle EnergyDonovan BlakeNessuna valutazione finora
- Janda ApproachDocumento5 pagineJanda ApproachMădălina StavaracheNessuna valutazione finora
- GX Annular Blowout PreventerDocumento2 pagineGX Annular Blowout PreventerCarlos Munizaga100% (1)
- Fascial Strain Counter Strain 2013Documento8 pagineFascial Strain Counter Strain 2013Rui Pedro PereiraNessuna valutazione finora
- L Kalichman PDFDocumento28 pagineL Kalichman PDFShahul HameedNessuna valutazione finora
- Self Myofascial ReleaseDocumento22 pagineSelf Myofascial ReleaseMuhammad Fahmy100% (1)
- Physiology and BiochemistryDa EverandPhysiology and BiochemistryGeoffrey BourneNessuna valutazione finora
- Strain and Counterstrain Cervical and Thoracic Tender Points GuideDocumento99 pagineStrain and Counterstrain Cervical and Thoracic Tender Points GuideD.O. dobirdNessuna valutazione finora
- Rolfing ConceptsDocumento14 pagineRolfing ConceptsFelipe Adriano100% (1)
- Neuro DynamicsDocumento26 pagineNeuro DynamicsRahul ChhatlaniNessuna valutazione finora
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocumento9 pagineApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinez100% (1)
- Chapman's Reflexes and Modern Clinical ApplicationsDocumento94 pagineChapman's Reflexes and Modern Clinical ApplicationsYuldash100% (1)
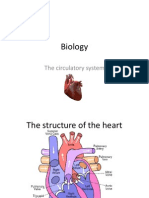
- Biology IGCSE Human Circulatory SystemDocumento17 pagineBiology IGCSE Human Circulatory SystemNiharika100% (1)
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocumento9 pagineApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinezNessuna valutazione finora
- Fascial Manipulation DescriptionDocumento7 pagineFascial Manipulation DescriptionPopescu MariusNessuna valutazione finora
- Essentials of o Ste 00 DaveDocumento112 pagineEssentials of o Ste 00 DaveGeki Iovan100% (1)
- Visceral OMT: AAO Convocation March 2018 Kenneth Lossing DODocumento59 pagineVisceral OMT: AAO Convocation March 2018 Kenneth Lossing DODiana SchlittlerNessuna valutazione finora
- Stecco Workshop Full Text PDFDocumento18 pagineStecco Workshop Full Text PDFsumarumNessuna valutazione finora
- Work at Height - ScaffoldingDocumento46 pagineWork at Height - ScaffoldingajayjanardhankasleNessuna valutazione finora
- Monster Hunter, DND 5.0. - Guild MonsterDocumento2 pagineMonster Hunter, DND 5.0. - Guild MonsterJuan Daniel EcheverriNessuna valutazione finora
- An Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Documento8 pagineAn Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Adolfo Esteban Soto MartinezNessuna valutazione finora
- Diagnostic Touch Parts I IV by Rollin Becker PDFDocumento69 pagineDiagnostic Touch Parts I IV by Rollin Becker PDFCatalin EneNessuna valutazione finora
- 10th DanDocumento5 pagine10th DanNilankan Betal0% (1)
- Fascial Training For More Flexibility, Suppleness and Vitality: This Is How You Get Your Fascias Into Top Form! (10 Minutes Fascia Workout For Home)Da EverandFascial Training For More Flexibility, Suppleness and Vitality: This Is How You Get Your Fascias Into Top Form! (10 Minutes Fascia Workout For Home)Nessuna valutazione finora
- Osteopathy in The Cranial FieldDocumento110 pagineOsteopathy in The Cranial FieldRukaphuongNessuna valutazione finora
- Visceral Anatomy For OsteopathyDocumento152 pagineVisceral Anatomy For OsteopathyHossein Khorrami100% (1)
- The Human Fascial System by L Stecco J A Day HandoutsDocumento4 pagineThe Human Fascial System by L Stecco J A Day Handoutsnyaniso rahotepNessuna valutazione finora
- Facilitated Positional Release FPRDocumento12 pagineFacilitated Positional Release FPRcoahuiltecoNessuna valutazione finora
- The Three LinksDocumento39 pagineThe Three Linksshaun goodmanNessuna valutazione finora
- Specifikasi Tadano GR-500XLDocumento11 pagineSpecifikasi Tadano GR-500XLHaka Surya GratamaNessuna valutazione finora
- Lecture Notes On Psoas & Adductors: Psoas As A Medial RotatorDocumento12 pagineLecture Notes On Psoas & Adductors: Psoas As A Medial RotatorAlisaClark100% (1)
- Godman - 1824 - Fascia of The Human BodyDocumento27 pagineGodman - 1824 - Fascia of The Human BodyDustin LimaNessuna valutazione finora
- Willey Studios Chelda Model 3 Sets 81 PDFDocumento5 pagineWilley Studios Chelda Model 3 Sets 81 PDFTracyNessuna valutazione finora
- Main Fuel Pump Overhauling Procedure Step-by-StepDocumento5 pagineMain Fuel Pump Overhauling Procedure Step-by-StepAnoop Vijayakumar100% (1)
- WWW Pokemoncoders Com Pokemon Fire Red Gameshark CodesDocumento20 pagineWWW Pokemoncoders Com Pokemon Fire Red Gameshark Codesiop deva0% (1)
- Gameweek 2 28 September 2021 PSG Manchester CityDocumento24 pagineGameweek 2 28 September 2021 PSG Manchester CityBen SaadNessuna valutazione finora
- Uam-Vertical Science9Documento23 pagineUam-Vertical Science9Daryl FCNessuna valutazione finora
- Land Cruiser V8 Towbar Wiring Kit InstallDocumento31 pagineLand Cruiser V8 Towbar Wiring Kit InstallVladimir TereshchenkoNessuna valutazione finora
- AudiDocumento21 pagineAudiapi-281175594Nessuna valutazione finora
- Five Nights at FreddyDocumento46 pagineFive Nights at Freddyapi-28960625675% (4)
- Proteção 03Documento1 paginaProteção 03Larisse CarvalhoNessuna valutazione finora
- Ingles Febrero 6to PrimariaDocumento26 pagineIngles Febrero 6to PrimariaVitia Arely Zuñiga RivasNessuna valutazione finora
- Automotive Systems and Components GuideDocumento5 pagineAutomotive Systems and Components GuideManiKjNessuna valutazione finora
- Despiece Yamaha XJR 1300cc - 5WM1 - 2003 PDFDocumento75 pagineDespiece Yamaha XJR 1300cc - 5WM1 - 2003 PDFJohann WolfgangNessuna valutazione finora
- New Job DSKDocumento804 pagineNew Job DSKdestaNessuna valutazione finora
- McPherson v. Tennessee Football, Inc. - Document No. 1Documento4 pagineMcPherson v. Tennessee Football, Inc. - Document No. 1Justia.comNessuna valutazione finora
- Field demo competition criteriaDocumento2 pagineField demo competition criteriaErl Ongcoy SorianoNessuna valutazione finora
- Oven PengeringDocumento32 pagineOven PengeringDwikiNessuna valutazione finora
- Tabla Prueba IvtDocumento6 pagineTabla Prueba IvtPabloFabianPucheCeaNessuna valutazione finora
- Hand Goniometry 1565417609716Documento19 pagineHand Goniometry 1565417609716AVIMANNU SINGHNessuna valutazione finora
- Washington Nationals (3-2) at Philadelphia Phillies (2-3)Documento4 pagineWashington Nationals (3-2) at Philadelphia Phillies (2-3)ascomakNessuna valutazione finora