Potrebbero piacerti anche
- The Clinical Utility of Zonulin Testing - Kresser InstituteDocumento3 pagineThe Clinical Utility of Zonulin Testing - Kresser Institutekandarpvyasa5930Nessuna valutazione finora
- The Hiv AIDS Charity For LifeDocumento12 pagineThe Hiv AIDS Charity For Lifekandarpvyasa5930Nessuna valutazione finora
- PR4100 Microplate Reader User Manual Pages 1 - 50 - Text Version - FlipHTML5 PDFDocumento224 paginePR4100 Microplate Reader User Manual Pages 1 - 50 - Text Version - FlipHTML5 PDFkandarpvyasa5930Nessuna valutazione finora
- Manual On Quality Standads For HIV Testing Laboratories PDFDocumento137 pagineManual On Quality Standads For HIV Testing Laboratories PDFkandarpvyasa5930Nessuna valutazione finora
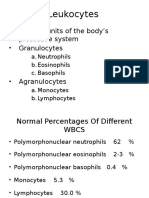
- WBCs 1Documento21 pagineWBCs 1kandarpvyasa5930Nessuna valutazione finora
- Using Conditional Formatting To Highlight Positives, or Any Sample of InterestDocumento3 pagineUsing Conditional Formatting To Highlight Positives, or Any Sample of Interestkandarpvyasa5930Nessuna valutazione finora
- Male Reproductive System: Related Kidshealth LinksDocumento7 pagineMale Reproductive System: Related Kidshealth Linkskandarpvyasa5930Nessuna valutazione finora
- IgG Vs IgE PDFDocumento2 pagineIgG Vs IgE PDFkandarpvyasa5930Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 13 Aseptic TechniqueDocumento6 pagine13 Aseptic TechniqueaironmaeNessuna valutazione finora
- Gingival Finish LinesDocumento15 pagineGingival Finish LinesAME DENTAL COLLEGE RAICHUR, KARNATAKANessuna valutazione finora
- CBQ Legal Ethical MNGTDocumento23 pagineCBQ Legal Ethical MNGTyzak jouleNessuna valutazione finora
- Depression Interview QuestionsDocumento3 pagineDepression Interview QuestionsStarlin Vijay Mythri100% (1)
- Cervical ExerciseDocumento16 pagineCervical ExerciseAmit Shukla100% (2)
- Chemotherapeutic Agents and AntiinfectivesDocumento64 pagineChemotherapeutic Agents and AntiinfectivesAnthony RiggsNessuna valutazione finora
- Angiography EquipmentDocumento60 pagineAngiography EquipmentKarthika UmashankarNessuna valutazione finora
- NCP (Fatigue)Documento3 pagineNCP (Fatigue)Edrick SilvaNessuna valutazione finora
- What Is A Case Study?: Roberta Heale, Alison TwycrossDocumento2 pagineWhat Is A Case Study?: Roberta Heale, Alison TwycrossBianca Benj ZariNessuna valutazione finora
- Mini EssayDocumento1 paginaMini EssayNonny Tentia MNessuna valutazione finora
- The Strange and Beautiful Sorrows of Ava Lavender by Leslye Walton - PrologueDocumento10 pagineThe Strange and Beautiful Sorrows of Ava Lavender by Leslye Walton - PrologueWalker BooksNessuna valutazione finora
- Vitamin K Administration in The Newborn GuidelineDocumento10 pagineVitamin K Administration in The Newborn GuidelineAna Sarah KurniaNessuna valutazione finora
- Catatonia PDFDocumento9 pagineCatatonia PDFDanilo RibeiroNessuna valutazione finora
- Antenatal SteroidsDocumento30 pagineAntenatal Steroidskhadzx100% (2)
- 940837-000001 LMA-Protector Factsheet 1604Documento2 pagine940837-000001 LMA-Protector Factsheet 1604nanang criztaNessuna valutazione finora
- Symptoms of Nasal PolypsDocumento5 pagineSymptoms of Nasal Polypspratik hamalNessuna valutazione finora
- 10 Rights in Drug AdministrationDocumento25 pagine10 Rights in Drug AdministrationNathaniel PulidoNessuna valutazione finora
- Post TestDocumento11 paginePost TestDemuel Dee L. BertoNessuna valutazione finora
- Neural Retraining Project Highlights: Completion of First Phase Informs Creation of Clinical Trials ProtocolDocumento2 pagineNeural Retraining Project Highlights: Completion of First Phase Informs Creation of Clinical Trials ProtocolDeepak RanaNessuna valutazione finora
- Charcot JointDocumento8 pagineCharcot JointAtika SugiartoNessuna valutazione finora
- CPR PDFDocumento37 pagineCPR PDFArdhi AgustjikNessuna valutazione finora
- Gastritis PPTDocumento86 pagineGastritis PPTWayan Hery75% (4)
- Meningitis-Malaria E PDFDocumento44 pagineMeningitis-Malaria E PDFSana ShafeeqNessuna valutazione finora
- Research # 1: Laguna State Polytechnic UniversityDocumento10 pagineResearch # 1: Laguna State Polytechnic UniversityAbigael Patricia GutierrezNessuna valutazione finora
- Agencies WebsitesDocumento4 pagineAgencies WebsitesWWMTNessuna valutazione finora
- Headsss 3.0 &Phq9Documento39 pagineHeadsss 3.0 &Phq9Charity Asprer OsorioNessuna valutazione finora
- CHOLANGIOCARCINOMADocumento26 pagineCHOLANGIOCARCINOMAPremaKurnia100% (3)
- Nail ExtractionDocumento5 pagineNail ExtractionArip SeptadiNessuna valutazione finora
- Ranitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDocumento6 pagineRanitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDewi Wara ShintaNessuna valutazione finora
- Multiple Choice Question (MCQ) Exam: 15 Sample QuestionsDocumento4 pagineMultiple Choice Question (MCQ) Exam: 15 Sample QuestionsAnkita AgarwallNessuna valutazione finora