Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Talenta MudaDocumento4 pagineTalenta MudaLanna HarumiyaNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- ValdesDocumento4 pagineValdesLanna HarumiyaNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- TroubleDocumento4 pagineTroubleLanna HarumiyaNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Teepe 2015Documento4 pagineTeepe 2015Lanna HarumiyaNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- GENDUTDocumento11 pagineGENDUTLanna HarumiyaNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Dinosaurus XXXXXXXDocumento4 pagineDinosaurus XXXXXXXLanna HarumiyaNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- EclipseDocumento5 pagineEclipsejeevanpbNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- MinimalismDocumento8 pagineMinimalismLanna HarumiyaNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Presentation TitleDocumento4 paginePresentation TitleLanna HarumiyaNessuna valutazione finora
- Biophysical Characterization of Dry Facial Skin: J. L. Leveque, G. Grove, J. de Rigal, P. CorcuffDocumento8 pagineBiophysical Characterization of Dry Facial Skin: J. L. Leveque, G. Grove, J. de Rigal, P. CorcuffLanna HarumiyaNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Baweja2010 PDFDocumento14 pagineBaweja2010 PDFLanna HarumiyaNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Life Without KaplanDocumento8 pagineLife Without KaplanLanna HarumiyaNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- DownloadDocumento5 pagineDownloadLanna HarumiyaNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Nouveau Richard 2007Documento6 pagineNouveau Richard 2007Lanna HarumiyaNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Gloomy LifeDocumento6 pagineGloomy LifeLanna HarumiyaNessuna valutazione finora
- Single Agent Gemcitabine Chemotherapy in Dogs With Spontaneously Occurring LymphomaDocumento5 pagineSingle Agent Gemcitabine Chemotherapy in Dogs With Spontaneously Occurring LymphomaLanna HarumiyaNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- 10 0000@Www Jstage JST Go jp@Article@Jat@23@11@2335436@ArticleDocumento9 pagine10 0000@Www Jstage JST Go jp@Article@Jat@23@11@2335436@ArticleLanna HarumiyaNessuna valutazione finora
- Click To Edit Master Subtitle StyleDocumento4 pagineClick To Edit Master Subtitle StyleLanna HarumiyaNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Single Agent Gemcitabine Chemotherapy in Dogs With Spontaneously Occurring LymphomaDocumento5 pagineSingle Agent Gemcitabine Chemotherapy in Dogs With Spontaneously Occurring LymphomaLanna HarumiyaNessuna valutazione finora
- Tentative Acara Workshop SimpoDocumento7 pagineTentative Acara Workshop SimpoLanna HarumiyaNessuna valutazione finora
- Click To Edit Master Title StyleDocumento4 pagineClick To Edit Master Title StyleLanna HarumiyaNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Click To Edit Master Subtitle StyleDocumento4 pagineClick To Edit Master Subtitle StyleLanna HarumiyaNessuna valutazione finora
- Title: SubheadingDocumento7 pagineTitle: SubheadingLanna HarumiyaNessuna valutazione finora
- Kol Ditz 2016Documento3 pagineKol Ditz 2016Lanna HarumiyaNessuna valutazione finora
- Frans Sarumpaet, Dr. Pembimbing: Bayu Rusfandi, DR., SPPDDocumento13 pagineFrans Sarumpaet, Dr. Pembimbing: Bayu Rusfandi, DR., SPPDLanna HarumiyaNessuna valutazione finora
- Leprosi UlcerDocumento7 pagineLeprosi UlcerLanna HarumiyaNessuna valutazione finora
- PPDS Pti, OkDocumento2 paginePPDS Pti, OkLanna HarumiyaNessuna valutazione finora
- Chest TubeDocumento34 pagineChest TubeLanna HarumiyaNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Barrera 2016Documento10 pagineBarrera 2016Lanna HarumiyaNessuna valutazione finora
- Sample Final Exam Questions-f14-KEYDocumento6 pagineSample Final Exam Questions-f14-KEYAlias HedgeNessuna valutazione finora
- Kode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Documento10 pagineKode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Dini AzizahNessuna valutazione finora
- Anaemia in Pregnancy: Klinik Kesihatan Ibu Dan Anak Parit BuntarDocumento10 pagineAnaemia in Pregnancy: Klinik Kesihatan Ibu Dan Anak Parit Buntarannurshah05Nessuna valutazione finora
- Benign Breast DiseasesDocumento35 pagineBenign Breast DiseasesBhim Nath KharelNessuna valutazione finora
- Definitive Guide To Red Light Therapy PhotobiomodulationDocumento10 pagineDefinitive Guide To Red Light Therapy PhotobiomodulationDavid Jenkins0% (2)
- Diabetis 2Documento33 pagineDiabetis 2Fercho MedNessuna valutazione finora
- Broiler Breeder DiseasesDocumento12 pagineBroiler Breeder DiseasesvetbcasNessuna valutazione finora
- Consensus Based Guidelines For The Recognition,.15Documento13 pagineConsensus Based Guidelines For The Recognition,.15ms98alissaNessuna valutazione finora
- Grading Breast Camod Path2000Documento6 pagineGrading Breast Camod Path2000Dima PathNessuna valutazione finora
- Full-Sentence Speech FinalDocumento2 pagineFull-Sentence Speech Finalapi-363883917Nessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Limping Child: Department of Orthopaedics Afmc, PuneDocumento101 pagineLimping Child: Department of Orthopaedics Afmc, Punerithesh ramachandranNessuna valutazione finora
- Neonatal Respiratory DistressDocumento59 pagineNeonatal Respiratory DistressMohamad Saleh100% (7)
- Mi (Case # 1) : 1. How Would You Classify Mr. Smith's Chest Pain?Documento11 pagineMi (Case # 1) : 1. How Would You Classify Mr. Smith's Chest Pain?Faizan MazharNessuna valutazione finora
- Slides From McCullough 10-27-2021 PresentationDocumento83 pagineSlides From McCullough 10-27-2021 PresentationAssociation of American Physicians and Surgeons100% (10)
- Homeopathy Cases by KadwaDocumento179 pagineHomeopathy Cases by Kadwaabckadwa100% (3)
- Clinical Learning Log 3 Go Solo - Docx-1Documento11 pagineClinical Learning Log 3 Go Solo - Docx-1JezraleFame AntoyNessuna valutazione finora
- Paedia - Dr. RehabDocumento173 paginePaedia - Dr. RehabMohammed Saad NabhanNessuna valutazione finora
- RetinaDocumento19 pagineRetinaSuze C.Nessuna valutazione finora
- Buttaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Documento3 pagineButtaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Vivian ChanNessuna valutazione finora
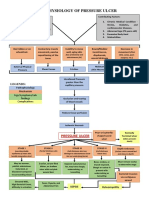
- Pathophysiology of Pressure UlcerDocumento1 paginaPathophysiology of Pressure UlcerSTORAGE FILENessuna valutazione finora
- PediatricsDocumento21 paginePediatricsManoj KumarNessuna valutazione finora
- "Oral Questions in Clinical Surgery" Case 1. LipomaDocumento19 pagine"Oral Questions in Clinical Surgery" Case 1. LipomaSherif Magdi100% (3)
- Klinefelter Syndrome in Clinical Practice. Nat Clin Pract Urol 4:192-204Documento14 pagineKlinefelter Syndrome in Clinical Practice. Nat Clin Pract Urol 4:192-204Anonymous LAWfm7Nessuna valutazione finora
- Endocrine NCLEX PN Pract & ANS Questions IIDocumento13 pagineEndocrine NCLEX PN Pract & ANS Questions IIYA HONessuna valutazione finora
- What Is Heart Bypass SurgeryDocumento10 pagineWhat Is Heart Bypass SurgeryVanitha AlagarsamyNessuna valutazione finora
- Pathological Repertory of The NosodesDocumento20 paginePathological Repertory of The Nosodespawajee100% (1)
- Data Lens Overview: Category Keyword CountDocumento25 pagineData Lens Overview: Category Keyword CountHari HaranNessuna valutazione finora
- c22 Microbiology Tortora TestbankDocumento16 paginec22 Microbiology Tortora Testbankwhitewave25Nessuna valutazione finora
- Pathogenesis of Bacterial InfectionDocumento35 paginePathogenesis of Bacterial InfectionDiyantoro NyoNessuna valutazione finora
- Acute Suppurative Parotitis: Related SummariesDocumento7 pagineAcute Suppurative Parotitis: Related SummariesFarida Dwi IrnawatiNessuna valutazione finora
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerDa EverandGut: the new and revised Sunday Times bestsellerValutazione: 4 su 5 stelle4/5 (393)