Potrebbero piacerti anche
- Management of Multiple PregnancyDocumento14 pagineManagement of Multiple PregnancyxxdrivexxNessuna valutazione finora
- Journal Ectopic Pregnancy-A Rising TrendDocumento5 pagineJournal Ectopic Pregnancy-A Rising TrendEricNessuna valutazione finora
- Visceral Emergencies and Pregnancya Case Series of 11 Cases and Literature ReviewDocumento4 pagineVisceral Emergencies and Pregnancya Case Series of 11 Cases and Literature ReviewIJAR JOURNALNessuna valutazione finora
- Ectopic PregnancyDocumento24 pagineEctopic PregnancybertouwNessuna valutazione finora
- Management of Urinary Tract Infections in PregnancyDocumento26 pagineManagement of Urinary Tract Infections in PregnancySylvia WijayaNessuna valutazione finora
- Sagesorg-Guidelines For The Use of Laparoscopy During PregnancyDocumento32 pagineSagesorg-Guidelines For The Use of Laparoscopy During PregnancyLuis Acosta CumberbatchNessuna valutazione finora
- Early Warning ScoreDocumento28 pagineEarly Warning ScoreFahmi MaslanNessuna valutazione finora
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDocumento8 pagineAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyNessuna valutazione finora
- Guidelines For Good Practice in The Management of Neonatal Respiratory Distress SyndromeDocumento29 pagineGuidelines For Good Practice in The Management of Neonatal Respiratory Distress SyndromeMehul RanaNessuna valutazione finora
- Investigation and Management of MenorrhagiaDocumento26 pagineInvestigation and Management of MenorrhagiaRahdin Ahmad Faresy Al-HamidiNessuna valutazione finora
- Recurrent Pregnancy LossDocumento19 pagineRecurrent Pregnancy LossSean NamNessuna valutazione finora
- Management of Cervical CancerDocumento29 pagineManagement of Cervical CancersangheetaNessuna valutazione finora
- Cord ProlapseDocumento15 pagineCord Prolapsexxdrivexx67% (3)
- 1 PDFDocumento7 pagine1 PDFAlfa FebriandaNessuna valutazione finora
- RCOG Guidelines - Gestational Trophoblastic DiseaseDocumento12 pagineRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- Medication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1Documento77 pagineMedication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1doodrillNessuna valutazione finora
- Vaginal Delivery of Breech Presentation: Sogc Clinical Practice GuidelineDocumento10 pagineVaginal Delivery of Breech Presentation: Sogc Clinical Practice GuidelineSyifa Rakhmi SungaidiNessuna valutazione finora
- OB - 02 - Outcomes of Multifetal ReductionDocumento6 pagineOB - 02 - Outcomes of Multifetal Reductionram4a5Nessuna valutazione finora
- 1 s2.0 S0020729209615502 Main PDFDocumento1 pagina1 s2.0 S0020729209615502 Main PDFPaula UrsuNessuna valutazione finora
- NsaikilaDocumento14 pagineNsaikilaayafor eric pekwalekeNessuna valutazione finora
- Journal Gyn KETDocumento8 pagineJournal Gyn KETImaylani S. SitanggangNessuna valutazione finora
- Bakker 2012Documento10 pagineBakker 2012ieoNessuna valutazione finora
- Neonatal and Maternal Complications of Placenta Praevia and Its Risk Factors in Tikur Anbessa Specialized and Gandhi Memorial Hospitals. Unmatched Case-Control StudyDocumento10 pagineNeonatal and Maternal Complications of Placenta Praevia and Its Risk Factors in Tikur Anbessa Specialized and Gandhi Memorial Hospitals. Unmatched Case-Control StudyLarassati YayaNessuna valutazione finora
- Green Top Guidelines 11Documento24 pagineGreen Top Guidelines 11garfield1Nessuna valutazione finora
- Gui 288 CPG1303 EDocumento16 pagineGui 288 CPG1303 EDwitari Novalia HaraziNessuna valutazione finora
- Desi Rahayu (153112540120468Documento53 pagineDesi Rahayu (153112540120468Bella FebriyantiNessuna valutazione finora
- Comparative Study For Efficacy of Termination in First Trimester Pregnancy Using Misoprostol and MifepristoneDocumento9 pagineComparative Study For Efficacy of Termination in First Trimester Pregnancy Using Misoprostol and MifepristonePeertechz Publications Inc.Nessuna valutazione finora
- Pi Is 0020729213005055Documento4 paginePi Is 0020729213005055Winna Eka PNessuna valutazione finora
- ANESTHESIOLOGY (R) 2016 - Refresher Course Lecture Summaries副本(被拖移)Documento9 pagineANESTHESIOLOGY (R) 2016 - Refresher Course Lecture Summaries副本(被拖移)Han biaoNessuna valutazione finora
- Proforma For Registration of Subjects For Dissertation: I Year M. SC Nursing Obstetrics and Gynecology YEAR 2007-2009Documento19 pagineProforma For Registration of Subjects For Dissertation: I Year M. SC Nursing Obstetrics and Gynecology YEAR 2007-2009savitaNessuna valutazione finora
- Gynecology & Reproductive HealthDocumento6 pagineGynecology & Reproductive HealthtiaranindyNessuna valutazione finora
- Protocolo CanadaDocumento5 pagineProtocolo Canadashluly23Nessuna valutazione finora
- The Long Acting Reversible Contraceptive (LARC) GuidelineDocumento20 pagineThe Long Acting Reversible Contraceptive (LARC) GuidelineYinlerLeeNessuna valutazione finora
- ProtocolDocumento30 pagineProtocolYousuf SawdagorNessuna valutazione finora
- RCPI Management of Early Pregnancy MiscarriageDocumento24 pagineRCPI Management of Early Pregnancy MiscarriagerazorazNessuna valutazione finora
- Diagnosis and Management of Ectopic Pregnancy-A Basic View Through LiteratureDocumento2 pagineDiagnosis and Management of Ectopic Pregnancy-A Basic View Through LiteraturefprasasyaaNessuna valutazione finora
- DTSCH Arztebl Int-112-0693 PDFDocumento13 pagineDTSCH Arztebl Int-112-0693 PDFKhoirunnisaSPazkaNessuna valutazione finora
- Abortion PDFDocumento7 pagineAbortion PDFAzrin AgmalinaNessuna valutazione finora
- Study of Management in Patient With Ectopic Pregnancy: Key WordsDocumento3 pagineStudy of Management in Patient With Ectopic Pregnancy: Key WordsparkfishyNessuna valutazione finora
- Peripartum Hystrectomy - 2 Year Retrospective Clinical Study I Regional Institute of Medical Sciences Imphal ManipurDocumento11 paginePeripartum Hystrectomy - 2 Year Retrospective Clinical Study I Regional Institute of Medical Sciences Imphal ManipurIOSRjournalNessuna valutazione finora
- Acog Practice Bulletin: Early Pregnancy LossDocumento11 pagineAcog Practice Bulletin: Early Pregnancy LossAlberto Kenyo Riofrio PalaciosNessuna valutazione finora
- Investigation and Management of Late Fetal Intrauterine Death and StillbirthDocumento64 pagineInvestigation and Management of Late Fetal Intrauterine Death and StillbirthDFsawlNessuna valutazione finora
- Challenges in The Management of A Case of 2nd Abdominal Pregnancy - OJOG - 2015092815302981Documento3 pagineChallenges in The Management of A Case of 2nd Abdominal Pregnancy - OJOG - 2015092815302981Stella Putri WandaNessuna valutazione finora
- No. 373-Cervical Insuf Ficiency and Cervical Cerclage: Sogc Clinical Practice GuidelineDocumento15 pagineNo. 373-Cervical Insuf Ficiency and Cervical Cerclage: Sogc Clinical Practice GuidelineGusti Paramartha100% (1)
- Article 233230Documento11 pagineArticle 233230arreyemilieneNessuna valutazione finora
- Maternal and Perinatal Outcomes After Elective Labor Induction at 39 Weeks in Uncomplicated Singleton Pregnancies - A Meta-Analysis-sotiriadis2018Documento27 pagineMaternal and Perinatal Outcomes After Elective Labor Induction at 39 Weeks in Uncomplicated Singleton Pregnancies - A Meta-Analysis-sotiriadis2018trongnguyen2232000Nessuna valutazione finora
- (Sici) 1097 0215 (19970529) 71 5 800 Aid Ijc18 3.0Documento7 pagine(Sici) 1097 0215 (19970529) 71 5 800 Aid Ijc18 3.0Moh RamliNessuna valutazione finora
- BMJ f6398Documento13 pagineBMJ f6398Luis Gerardo Pérez CastroNessuna valutazione finora
- Care in Pregnancies Subsequent To Stillbirthor Perinatal DeatDocumento12 pagineCare in Pregnancies Subsequent To Stillbirthor Perinatal DeatgalalNessuna valutazione finora
- Obstetrics & Gynecology: Course ObjectivesDocumento3 pagineObstetrics & Gynecology: Course Objectivespavi7muruganathanNessuna valutazione finora
- Brewer 2011Documento17 pagineBrewer 2011Iman BousnaneNessuna valutazione finora
- Ectopic Pregnancy Risk Factors, Clinical Presentation and ManagementDocumento6 pagineEctopic Pregnancy Risk Factors, Clinical Presentation and ManagementRizka AdiNessuna valutazione finora
- WHO Recommendation On Techniques For Preventing Perineal Trauma During Labour - RHL PDFDocumento19 pagineWHO Recommendation On Techniques For Preventing Perineal Trauma During Labour - RHL PDFsaksNessuna valutazione finora
- Evidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFDocumento16 pagineEvidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFErika GuerreroNessuna valutazione finora
- Obstetrics Gynecology Competencies e PDFDocumento22 pagineObstetrics Gynecology Competencies e PDFمركز ريلاكس للعلاج الطبيعيNessuna valutazione finora
- CVX Length SOGCDocumento14 pagineCVX Length SOGCBrendaNessuna valutazione finora
- Gui 233 CPG0909Documento5 pagineGui 233 CPG0909kyle31100% (1)
- Management of Infertility: A Practical ApproachDa EverandManagement of Infertility: A Practical ApproachAntonio Simone LaganàNessuna valutazione finora
- Clinical Pharmacology During PregnancyDa EverandClinical Pharmacology During PregnancyDonald MattisonNessuna valutazione finora
- Resuscitation For The Pregnant WomanDocumento18 pagineResuscitation For The Pregnant WomanxxdrivexxNessuna valutazione finora
- Nutrition in PregnancyDocumento15 pagineNutrition in PregnancyxxdrivexxNessuna valutazione finora
- Irish Maternity Early Warning System (IMEWS)Documento27 pagineIrish Maternity Early Warning System (IMEWS)xxdrivexxNessuna valutazione finora
- Management of Breech PresentationDocumento26 pagineManagement of Breech PresentationxxdrivexxNessuna valutazione finora
- Management of Pelvic Girdle Pain in Pregnancy and Post-PartumDocumento27 pagineManagement of Pelvic Girdle Pain in Pregnancy and Post-PartumxxdrivexxNessuna valutazione finora
- Nutrition During PregnancyDocumento48 pagineNutrition During PregnancyxxdrivexxNessuna valutazione finora
- Ultrasound Diagnosis of Early Pregnancy LossDocumento18 pagineUltrasound Diagnosis of Early Pregnancy LossxxdrivexxNessuna valutazione finora
- Obesity and PregnancyDocumento39 pagineObesity and PregnancyxxdrivexxNessuna valutazione finora
- Tocolytic Treatment in PregnancyDocumento21 pagineTocolytic Treatment in PregnancyxxdrivexxNessuna valutazione finora
- Cord ProlapseDocumento15 pagineCord Prolapsexxdrivexx67% (3)
- Listeriosis in PregnancyDocumento18 pagineListeriosis in PregnancyxxdrivexxNessuna valutazione finora
- View Public Profile Find All Posts by Samsa Find All Threads Started by SamsaDocumento5 pagineView Public Profile Find All Posts by Samsa Find All Threads Started by SamsaxxdrivexxNessuna valutazione finora
- Medical Surgical Nursing Assignment - 2Documento147 pagineMedical Surgical Nursing Assignment - 2Sonali Sengar0% (1)
- Certain Conditions Originating in The Perinatal PeriodDocumento4 pagineCertain Conditions Originating in The Perinatal PeriodOlivia KristiantiNessuna valutazione finora
- Making Pregnancy Safer Safer Pregnancy in Tamil NaduDocumento100 pagineMaking Pregnancy Safer Safer Pregnancy in Tamil NaduUthayakumar KasthuriNessuna valutazione finora
- PIHDocumento12 paginePIHAnonymous pt6eA0100% (1)
- The Evolving Role of Midwives As Laborists: Original ReviewDocumento8 pagineThe Evolving Role of Midwives As Laborists: Original Reviewmnazri98Nessuna valutazione finora
- Role Play: Gastritic: Make An A VoitmentDocumento3 pagineRole Play: Gastritic: Make An A VoitmentGita MirnawatiNessuna valutazione finora
- Cavity Design Class IV Composite ResinDocumento6 pagineCavity Design Class IV Composite ResinelokfaiqNessuna valutazione finora
- Abdominal CT and TransVag UTZDocumento6 pagineAbdominal CT and TransVag UTZWeng Villaverde PampoNessuna valutazione finora
- SEMINAR ON MULTIPLE PREGNANCY ContentDocumento21 pagineSEMINAR ON MULTIPLE PREGNANCY ContentMonika shankar0% (1)
- Self-Directed Learning (Nur 146 - Clinical Area)Documento2 pagineSelf-Directed Learning (Nur 146 - Clinical Area)Dyan Bianca Suaso LastimosaNessuna valutazione finora
- Functional Dyspepsia in ChildrenDocumento13 pagineFunctional Dyspepsia in ChildrenTimothy Eduard A. SupitNessuna valutazione finora
- Physicians 10-2022Documento38 paginePhysicians 10-2022PRC BaguioNessuna valutazione finora
- Anatomy and Physiology of Female Reproductive System:: VaginaDocumento5 pagineAnatomy and Physiology of Female Reproductive System:: VaginaphallicNessuna valutazione finora
- Review of The Physical Features FasdDocumento10 pagineReview of The Physical Features FasdSpencer Eduardo Alcayaga OlguínNessuna valutazione finora
- Step 2 NotesDocumento202 pagineStep 2 NotesNaved Rahman100% (2)
- Marcus Soos Accident April 19Documento3 pagineMarcus Soos Accident April 19api-310805543Nessuna valutazione finora
- The Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPDocumento32 pagineThe Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPAtri AmmuluNessuna valutazione finora
- Ramos v. Court of Appeals, G.R. No. 124354 December 29, 1999 Decision On MR, April 11, 2002Documento2 pagineRamos v. Court of Appeals, G.R. No. 124354 December 29, 1999 Decision On MR, April 11, 2002Pia SottoNessuna valutazione finora
- Amenorrhea Ovarian TumorsDocumento18 pagineAmenorrhea Ovarian TumorsJeremy ShimlerNessuna valutazione finora
- ULIPRISTALDocumento22 pagineULIPRISTALmeenakshi sundaramNessuna valutazione finora
- Physiotherapy For Women Obs PDFDocumento167 paginePhysiotherapy For Women Obs PDFvidyasagar pagilla100% (1)
- RAMOS-BN Drug Study Delivery RoomDocumento2 pagineRAMOS-BN Drug Study Delivery RoomLouwella RamosNessuna valutazione finora
- Gynaecological Ultrasound in Clinical Practice PDFDocumento247 pagineGynaecological Ultrasound in Clinical Practice PDFyulb_1Nessuna valutazione finora
- Pediatric Neuroanesthesia.3Documento4 paginePediatric Neuroanesthesia.3Mae Importers IncNessuna valutazione finora
- Medical Management of Missed AbortionDocumento4 pagineMedical Management of Missed AbortionJonathan San MartinNessuna valutazione finora
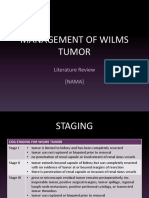
- Management of Wilms Tumor: Literature Review (NAMA)Documento15 pagineManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaNessuna valutazione finora
- Filed Under: Multifocal Atrial TachycardiaDocumento3 pagineFiled Under: Multifocal Atrial TachycardiaBogdan TeoNessuna valutazione finora
- Baby Walker PDFDocumento2 pagineBaby Walker PDFNorhafizah AhmadNessuna valutazione finora
- Test 5 Answer KeyDocumento4 pagineTest 5 Answer KeyEliNessuna valutazione finora
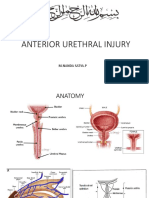
- Rupture Urethra Anterior DR Sule FixDocumento36 pagineRupture Urethra Anterior DR Sule FixkadinfathiaNessuna valutazione finora